Quick Summary: Machine learning is transforming medical imaging by enabling automated detection, diagnosis, and analysis of medical images with unprecedented accuracy. ML algorithms assist radiologists in identifying patterns in X-rays, MRIs, CT scans, and other imaging modalities, improving diagnostic speed and precision. The FDA has cleared numerous AI-enabled medical devices, with recent approvals marking significant milestones in clinical adoption.
Medical imaging has always been the cornerstone of modern diagnostics. But here’s the thing—radiologists face mounting pressures. Image volumes keep climbing. Diagnostic complexity increases. And the demand for faster, more accurate reads shows no signs of slowing.
Machine learning offers a path forward. By training algorithms on vast datasets of medical images, researchers have developed systems that can detect patterns invisible to the human eye, flag anomalies in seconds, and assist clinicians in rendering more confident diagnoses.
This isn’t science fiction. The FDA has cleared multiple AI-enabled medical imaging devices in late 2025, including devices like TruSPECT Processing Station and others in late 2025. These regulatory milestones signal that ML in medical imaging has moved from experimental labs into clinical reality.
What Is Machine Learning in Medical Imaging?
Machine learning represents a subset of artificial intelligence where algorithms learn from data rather than following explicit programming instructions. In medical imaging, ML systems analyze thousands or millions of images to identify patterns, make predictions, and support diagnostic decisions.
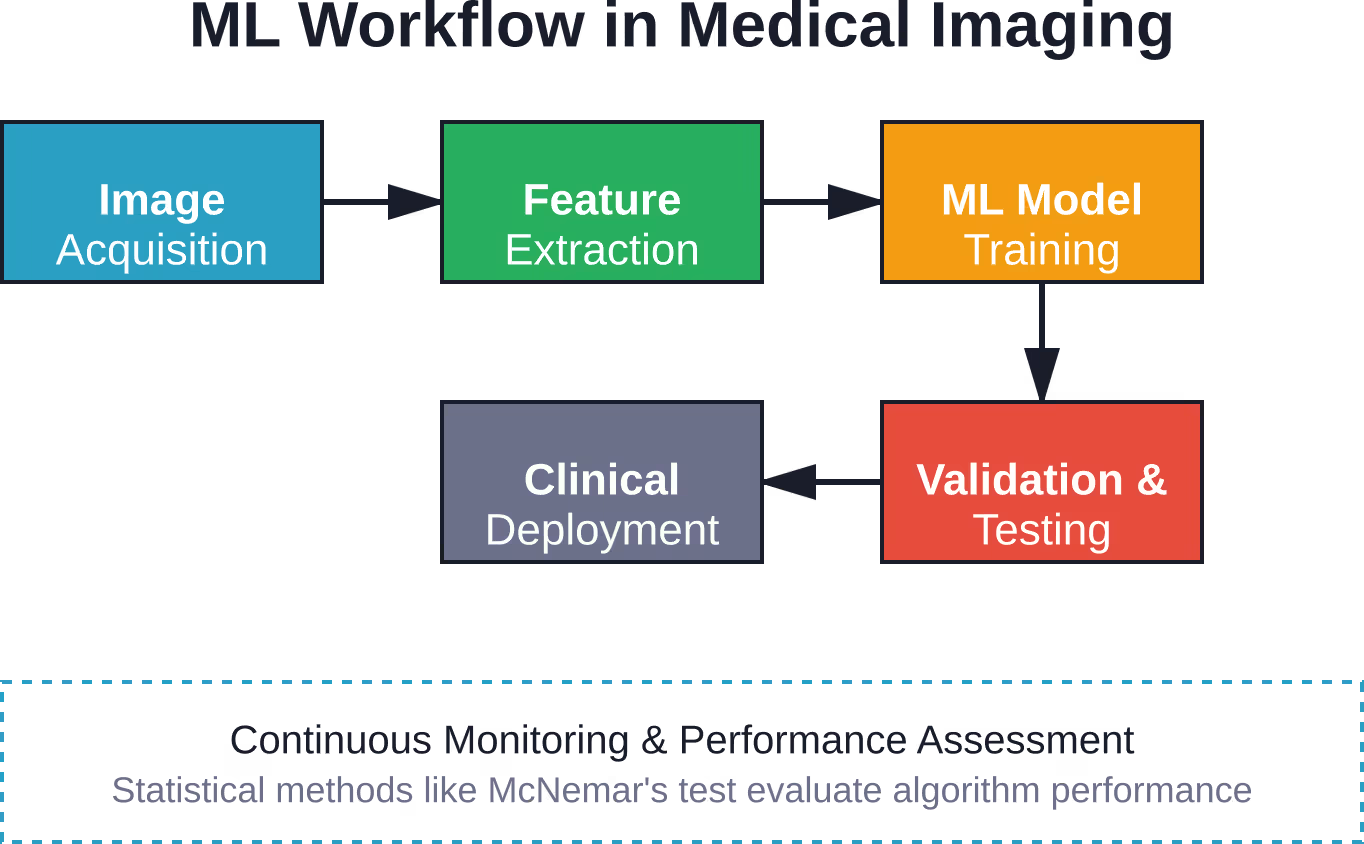
The process typically begins with feature extraction—the ML algorithm computes characteristics from images such as texture, shape, intensity patterns, and spatial relationships. These features feed into classification models that can distinguish between normal and abnormal findings, identify specific pathologies, or predict disease progression.
Research published by the National Institutes of Health demonstrates how ML algorithms can be overlaid onto whole-body MRI scans in the form of threshold, colored probability maps, or heatmaps. Radiologists determine the overlay threshold—often suggested at 65%—to balance sensitivity and specificity in their reads.
Core ML Techniques Applied to Medical Images
Several ML approaches dominate medical imaging applications:
- Support Vector Machines (SVM): Maximum-margin classifiers that separate different diagnostic categories in high-dimensional feature spaces
- Deep Learning Networks: Convolutional neural networks that automatically learn hierarchical features from raw image pixels
- Random Forests: Ensemble methods combining multiple decision trees for robust classification
- Reinforcement Learning: Emerging approaches for landmark detection, image segmentation, and sequential decision tasks
According to NIH research, microcalcifications appear as bright spots in mammograms and represent important indicators of breast cancer, appearing in 30–50% of cases. Individual microcalcifications can be difficult to detect due to their small size and variable appearance—precisely the type of challenge where ML excels.

Develop AI Solutions for Medical Imaging With AI Superior
Medical imaging AI projects require accurate models and reliable system integration. AI Superior provides AI consulting, custom software development, and machine learning expertise for healthcare and computer vision projects.
Need a Team for Your Medical Imaging AI Project?
AI Superior can help with:
- Computer vision and image analysis
- Custom ML model development
- AI consulting and PoC development
- Integration into existing systems
👉Contact AI Superior to discuss your medical imaging AI project.
Clinical Applications Transforming Healthcare
ML applications span virtually every imaging modality and clinical specialty. Real talk: some applications have matured faster than others, but the breadth of innovation is remarkable.
Radiology and Diagnostic Imaging
Computer-aided detection (CADe) systems assist radiologists in identifying suspicious findings. Computer-aided diagnosis (CADx) systems go further, characterizing lesions and estimating malignancy probability.
The American College of Radiology’s Data Science Institute develops frameworks for implementing ML in radiology practice. Their Define-AI Directory catalogs detailed use cases for leveraging AI tools and resources across radiology subspecialties.
Content-based image retrieval (CBIR) represents another powerful application. These systems search large image databases to find cases visually similar to a current case, providing radiologists with relevant comparison examples that can inform diagnostic decisions.
Cardiovascular Imaging
Cardiovascular imaging devices with AI support have received FDA clearance. This reflects growing confidence in ML algorithms for assessing cardiac structure, function, and perfusion from echocardiograms, cardiac MRI, and CT angiography.
ML algorithms analyze wall motion abnormalities, calculate ejection fraction, quantify valve stenosis, and predict cardiovascular risk with increasing sophistication. These tools help cardiologists process complex imaging studies more efficiently while maintaining diagnostic accuracy.
Neuroimaging and Brain Analysis
Recent FDA clearances represent advances in neuroimaging analysis. ML methods excel at identifying subtle patterns in brain imaging associated with neurodegenerative diseases, psychiatric conditions, and traumatic injuries.
Research demonstrates how ML approaches describe Alzheimer’s disease prevalence across different stages by analyzing MRI patterns. The significant heterogeneity observed across studies reveals that demographic and setting characteristics impact prevalence estimates—precisely the type of complex relationship ML can model.
Functional brain mapping also benefits from ML. Algorithms can predict diagnostic performance, automatically assess image quality, and identify neural networks associated with specific cognitive tasks or disease states.
Oncology Imaging
Cancer detection and staging represent high-impact ML applications. According to NCBI research, whole-body MRI with diffusion-weighted imaging, supported by ML methods, helps stage patients with cancer. The ML output images overlay onto WB-MRI T2-weighted scans as threshold maps, colored probability maps, or heatmaps.
Radiologists using ML support can allocate reading time more efficiently. Studies show that experienced and inexperienced readers benefit from algorithmic assistance, though inter-rater agreement varies based on reader experience and algorithm design.
| Imaging Modality | Common ML Applications | Recent FDA Clearances |
|---|---|---|
| X-ray/Mammography | Microcalcification detection, lung nodule identification, fracture detection | Multiple CADe systems |
| CT Scanning | Lesion characterization, organ segmentation, treatment planning | AI-enabled devices for CT planning |
| MRI | Tumor staging, image reconstruction, tissue characterization | AI-enabled devices for MRI reconstruction |
| Nuclear Medicine | Image processing, quantification, quality enhancement | AI-enabled devices for nuclear medicine processing |
| Ultrasound | Cardiac function assessment, fetal anomaly detection | AI-enabled ultrasound devices |
Validation Methods and Performance Assessment
Here’s where it gets interesting. ML algorithms can achieve impressive performance on development datasets but fail in real-world clinical settings. Rigorous validation separates research demonstrations from clinically useful tools.
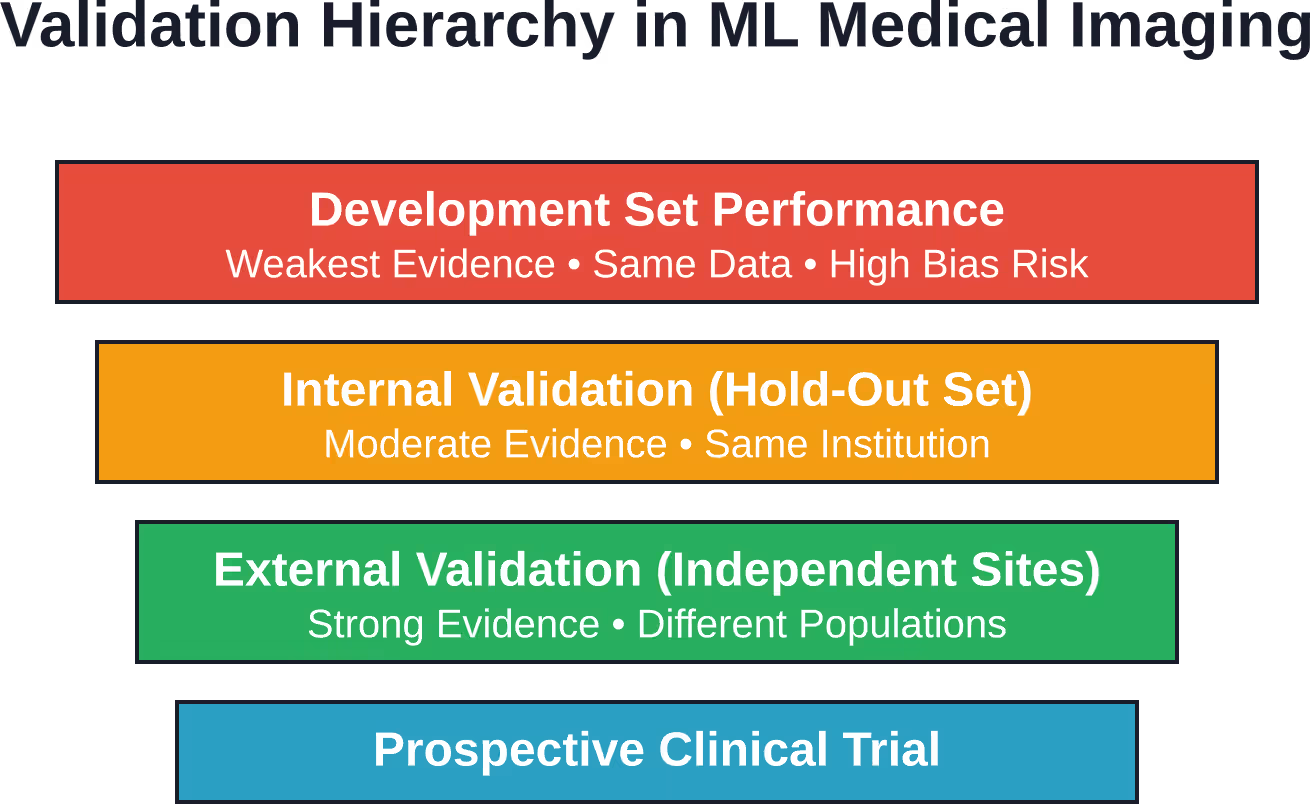
Internal vs External Validation
Internal validation tests algorithm performance on data from the same institution or study where it was developed. External validation—testing on completely independent datasets from different institutions, patient populations, or imaging equipment—provides stronger evidence of generalizability.
Research analyzing medical imaging ML studies reveals limited use of external validation and increased risk of bias across published articles. These methodological gaps present obstacles for clinical translation.
The FDA emphasizes appropriate evaluation methods for AI-enabled medical devices. Different intended applications require distinct performance metrics. Classification tasks use accuracy, sensitivity, and specificity. Regression tasks require mean absolute error or root mean squared error. Time-to-event predictions need concordance statistics.
Statistical Methods for Algorithm Comparison
When comparing ML-assisted reads to standard interpretation, McNemar’s test investigates differences in specificity rates between the two approaches. Studies report differences in proportions with 95% confidence intervals to quantify the magnitude and uncertainty of performance gains.
But wait. These statistical methods assume independence between samples. Paired reads on the same patients violate this assumption, requiring specialized statistical approaches that account for within-patient correlation.
The Challenge of Dataset Shift
ML models trained on one dataset often underperform when applied to new data with different characteristics. This phenomenon—called dataset shift or distribution shift—represents a fundamental challenge for medical imaging ML.
Analysis of Kaggle medical imaging challenges shows that the performance gap between public leaderboard sets and private test sets often exceeds the improvement between top-performing models. In other words, overfitting to the development set characteristics matters more than algorithmic refinements.
Regulatory Landscape and FDA Clearances
The FDA regulates AI-enabled medical devices through existing frameworks for Software as a Medical Device (SaMD). Medical device manufacturers using AI technologies must demonstrate safety and effectiveness through appropriate premarket submissions.
Recent Regulatory Milestones
The FDA has cleared multiple AI-enabled medical imaging devices in recent regulatory activity, including devices for nuclear medicine processing, MRI reconstruction, CT planning, and other applications across imaging modalities.
These clearances span multiple imaging modalities and clinical applications, demonstrating the breadth of ML deployment in medical imaging.
The FDA maintains an AI-Enabled Medical Device List identifying devices authorized for marketing in the United States. This resource helps digital health innovators understand the current device landscape and regulatory expectations. The list gets updated periodically but doesn’t represent a comprehensive catalog of all AI-enabled devices.
Evaluation Methods and Regulatory Expectations
The FDA’s Center for Devices and Radiological Health develops evaluation methods for AI-enabled medical devices. Different intended applications require distinct metrics for performance assessment.
Classification tasks (identifying whether a finding is present or absent) require metrics like sensitivity, specificity, positive predictive value, and negative predictive value. Regression tasks (estimating a continuous value like lesion size) need error metrics. Time-to-event predictions (survival analysis, disease progression) require appropriate statistical methods accounting for censored data.
The FDA encourages least burdensome approaches to evaluation. Developers should apply appropriate methods to each algorithm type rather than forcing standardized testing frameworks across diverse applications.
Quality Assurance Programs
The American College of Radiology’s ARCH-AI program represents the first national artificial intelligence quality assurance program for radiology facilities. It sets guidelines for AI use in imaging interpretation and recognizes facilities using AI safely and effectively.
The ACR-SIIM Practice Parameter for Imaging Artificial Intelligence defines operational and administrative requirements, personnel qualifications, and roles for implementing AI in radiology practices. Medical physicists play important roles in AI quality assurance alongside physicians and qualified end-users.
Methodological Challenges and Research Gaps
Despite impressive progress, systematic challenges slow advancement in medical imaging ML. Understanding these limitations helps set realistic expectations and prioritize research investments.
Data Limitations and Biases
Medical datasets, especially paired datasets of different modalities, lack the size and diversity needed for robust ML development. Training data often comes from single institutions serving specific patient populations, limiting generalizability.
Biases can creep in at every step. Selection bias affects which patients receive imaging. Measurement bias influences how images are acquired and interpreted. Label bias impacts the reference standards used to train algorithms. Publication bias skews the literature toward positive findings.
Research analyzing ML for medical imaging identifies these problems throughout the development pipeline. Data represents an imperfect window on clinical reality, and algorithms trained on biased data perpetuate or amplify those biases.
Evaluation That Misses the Target
Many ML studies optimize for metrics that don’t align with clinical utility. High area under the curve (AUC) values on test sets don’t guarantee improved patient outcomes, workflow efficiency, or cost-effectiveness.
The short answer? We need evaluation frameworks that measure what matters clinically. Does the algorithm reduce time to diagnosis? Does it improve diagnostic accuracy for challenging cases? Does it reduce unnecessary biopsies or additional imaging? Does it function reliably across diverse patient populations and imaging protocols?
These questions require prospective clinical studies, not just retrospective dataset analysis. The gap between algorithmic performance and clinical impact represents a critical research frontier.
Interpretability and Trust
Many high-performing ML models function as black boxes. Clinicians receive predictions without understanding the reasoning behind them. This opacity creates trust issues and makes error analysis difficult.
Frameworks for interpretability in ML medical imaging aim to make algorithm decisions more transparent. Attention maps, saliency visualizations, and feature importance rankings help clinicians understand which image regions drove specific predictions.
But interpretability involves tradeoffs. Simpler, more interpretable models sometimes sacrifice accuracy compared to complex deep learning architectures. Finding the right balance for each clinical application remains an active research area.
| Challenge Category | Specific Issues | Impact on Clinical Translation |
|---|---|---|
| Data Quality | Limited size, institutional bias, labeling errors, missing diversity | Algorithms underperform on new populations |
| Validation Rigor | Insufficient external testing, overfitting, dataset shift | Published performance overestimates real-world results |
| Evaluation Metrics | Metrics misaligned with clinical utility, lack of outcome data | Unclear whether algorithms improve patient care |
| Interpretability | Black-box predictions, limited explainability | Clinician distrust, difficult error analysis |
| Workflow Integration | Poor system interoperability, unclear roles and responsibilities | Adoption barriers despite proven accuracy |
Best Practices for ML Medical Imaging Development
Lessons from research failures and successes point toward evidence-based development practices that increase the likelihood of creating clinically useful tools.
Dataset Curation and Management
Start with clearly defined inclusion and exclusion criteria. Document patient demographics, imaging protocols, scanner models, and acquisition parameters. Assess whether the development dataset reflects the target clinical population.
Separate development, validation, and test sets rigorously. Data leakage between these sets—where information from the test set influences model development—represents a common source of overoptimistic performance estimates.
Seek diverse data sources. Multi-institutional collaborations produce more generalizable algorithms than single-center studies. If regulatory authorities and institutional review boards allow, consider data-sharing initiatives that expand training dataset diversity.
Algorithm Development and Training
Choose algorithms appropriate for the task. Not every problem requires deep learning. Simpler methods with good interpretability sometimes outperform complex architectures, especially with limited training data.
Implement rigorous cross-validation during development. Track performance on held-out validation sets throughout training to detect overfitting early. Monitor multiple metrics beyond accuracy—sensitivity, specificity, positive predictive value, and negative predictive value all provide important information.
Document hyperparameter choices, training procedures, and data augmentation strategies. Reproducibility requires detailed methodology that enables others to replicate and build upon published work.
Clinical Validation and Testing
Design validation studies that mirror intended clinical use. If the algorithm will support radiology reads, test it with radiologists interpreting images under realistic time constraints and workflow conditions.
Include appropriate statistical analyses. McNemar’s test with 95% confidence intervals provides standard methods for comparing paired diagnostic assessments. Consult biostatisticians during study design to ensure adequate sample sizes and appropriate statistical methods.
Measure reading time alongside diagnostic accuracy. Algorithms that improve accuracy but double reading time may not provide net clinical benefit. Those that maintain accuracy while reducing reading time could transform workflow efficiency.
Test across reader experience levels. Experienced and inexperienced readers may benefit differently from algorithmic support. Understanding these interactions helps target the tool to appropriate clinical contexts.
Regulatory Planning
Engage with regulatory authorities early. The FDA provides pre-submission programs where developers can discuss regulatory strategy before formal submissions. These consultations help identify appropriate evaluation methods and evidence requirements.
Determine the regulatory pathway. Most ML medical imaging devices pursue 510(k) clearance by demonstrating substantial equivalence to predicate devices. Novel applications may require De Novo classification or Premarket Approval.
Prepare comprehensive documentation. Marketing submissions for AI-enabled device software functions require extensive information supporting safety and effectiveness claims. Draft guidance documents outline recommended submission contents.
Comprehensive checklist spanning data curation, model training, validation testing, and clinical deployment phases of ML medical imaging development.
The Future of ML in Medical Imaging
Looking ahead, several trends will shape the next generation of ML medical imaging applications.
Multimodal Integration
Future systems will integrate information across imaging modalities, electronic health records, laboratory results, and genomic data. ML excels at finding patterns in high-dimensional heterogeneous data—perfect for multimodal medical information.
Paired datasets of different modalities remain limited in size and availability. Addressing this data scarcity through synthetic image translation represents one research direction. ML for medical image translation, particularly MRI to CT synthesis and vice versa, shows promise despite dataset limitations.
Reinforcement Learning Applications
Reinforcement learning has emerged as a powerful paradigm for complex decision-making tasks in medical image analysis. RL applications span landmark detection, image segmentation, lesion characterization, and sequential diagnostic workflows.
Unlike supervised learning, which requires extensive labeled training data, reinforcement learning algorithms learn through interaction with environments and reward signals. This approach may overcome some labeling bottlenecks that limit traditional ML development.
Federated Learning and Privacy Preservation
Training ML models without centralizing sensitive patient data addresses privacy concerns and enables larger, more diverse training datasets. Federated learning allows institutions to collaboratively train models while keeping data local.
This approach faces technical challenges around communication efficiency, model aggregation, and handling heterogeneous data distributions across sites. But the privacy benefits make it an attractive research direction as healthcare systems prioritize data protection.
Continuous Learning and Algorithm Updates
Medical imaging technology evolves rapidly. Scanner upgrades, protocol changes, and shifting patient populations can degrade algorithm performance over time. Static models trained once and deployed indefinitely won’t maintain optimal performance.
Continuous learning systems that update as new data becomes available represent the future. These systems require careful monitoring to detect when updates improve versus harm performance. Regulatory frameworks must evolve to accommodate algorithms that change post-deployment while maintaining safety oversight.
Implementation Considerations for Healthcare Systems
Adopting ML medical imaging tools requires more than purchasing software. Successful implementation demands careful planning across technical, clinical, and organizational dimensions.
Infrastructure Requirements
ML algorithms process large imaging datasets, requiring adequate computational resources. Some tools run on standard workstations. Others need dedicated GPU servers or cloud computing infrastructure.
System interoperability matters. Algorithms must integrate with existing PACS (picture archiving and communication systems), radiology information systems, and electronic health records. Standards like DICOM facilitate integration, but implementation details vary across vendors.
Workflow Integration
The best algorithm fails if clinicians can’t use it efficiently. ML tools should integrate seamlessly into existing radiology workflows, not create additional steps or delays.
Consider when algorithms present results. Pre-read flagging of urgent findings enables faster triage. Post-read second opinion functions help catch missed findings. Concurrent display during interpretation supports real-time decision-making. Each approach fits different clinical scenarios.
Training and Change Management
Radiologists need training to use ML tools effectively and understand their limitations. What types of findings does the algorithm detect reliably? Where does it struggle? How should clinicians interpret probability scores or colored overlays?
Change management extends beyond individual training. Departments must establish policies for algorithm use, define quality assurance procedures, and create governance structures for selecting and monitoring ML tools.
Quality Assurance and Monitoring
The ACR’s ARCH-AI program provides frameworks for quality assurance. Facilities should track algorithm performance continuously, not just during initial validation. Performance monitoring detects degradation over time or systematic errors in specific patient subgroups.
Establish clear escalation pathways for findings or algorithm failures. Define roles and responsibilities for medical physicists, IT staff, radiologists, and vendors in maintaining system performance.
Frequently Asked Questions
How accurate is machine learning in medical imaging compared to radiologists?
ML algorithm accuracy varies widely depending on the specific task, imaging modality, and clinical context. For some well-defined tasks like detecting microcalcifications in mammography, algorithms achieve sensitivity and specificity comparable to experienced radiologists. However, algorithms typically excel at narrow, specific tasks while radiologists demonstrate broader clinical reasoning. The most effective approach combines algorithmic support with radiologist expertise rather than replacing human interpretation entirely.
Are ML medical imaging devices FDA-approved?
Yes, the FDA has cleared numerous AI-enabled medical imaging devices through the 510(k) pathway and other regulatory mechanisms. The FDA has authorized multiple AI-enabled medical imaging devices for clinical use. The FDA maintains an AI-Enabled Medical Device List identifying authorized devices. Developers must demonstrate safety and effectiveness through appropriate premarket submissions with rigorous validation data.
What are the main challenges preventing wider adoption of ML in medical imaging?
Several barriers slow clinical adoption. Data limitations—including small dataset sizes, institutional biases, and lack of diversity—restrict algorithm generalizability. Methodological challenges around validation rigor and evaluation metrics make it difficult to assess true clinical utility. Integration difficulties with existing healthcare IT systems create implementation friction. Regulatory uncertainty for novel applications and concerns about liability also contribute. Finally, limited evidence demonstrating improved patient outcomes versus just algorithmic performance metrics slows adoption decisions.
Can machine learning algorithms work across different imaging equipment and protocols?
This represents a significant challenge called dataset shift. Algorithms trained on images from specific scanner models or acquisition protocols often underperform when applied to data from different equipment or settings. Research shows that performance degradation from development to external validation frequently exceeds the performance gap between competing algorithms. Developing robust algorithms requires training on diverse multi-institutional datasets spanning various scanners and protocols, though such datasets remain scarce.
How do radiologists use ML algorithm outputs in clinical practice?
Implementation varies by tool and clinical context. According to NCBI research, ML outputs overlay onto medical images as threshold maps, colored probability maps, or heatmaps. Radiologists can adjust visualization parameters like the overlay threshold—commonly set around 65%—to balance sensitivity and specificity based on clinical judgment. Some systems provide pre-read flagging of concerning findings for prioritization. Others offer second-read support to reduce missed findings. Radiologists integrate algorithmic suggestions with clinical history, additional imaging, and diagnostic reasoning to reach final interpretations.
What specialized training do healthcare professionals need to work with ML imaging tools?
Training requirements span technical, clinical, and quality assurance domains. Radiologists need education on algorithm capabilities, limitations, and appropriate interpretation of ML outputs. Medical physicists require expertise in algorithm validation, performance monitoring, and quality assurance procedures. IT professionals need skills in system integration, data management, and infrastructure support. The ACR-SIIM Practice Parameter for Imaging Artificial Intelligence defines qualifications and roles for various personnel. Organizations should establish ongoing education programs as ML technology evolves rather than one-time training sessions.
Will machine learning replace radiologists?
Industry consensus suggests augmentation rather than replacement. ML excels at specific pattern recognition tasks but lacks the broader clinical reasoning, communication skills, and judgment radiologists provide. Algorithms struggle with rare conditions, unusual presentations, and cases requiring integration of clinical context. The American College of Radiology envisions ML tools helping radiologists work more efficiently—enabling faster reads, reducing errors, and allowing focus on complex cases requiring expertise. The collaboration between human intelligence and machine learning likely produces better outcomes than either alone.
Conclusion
Machine learning has moved from experimental research to clinical reality in medical imaging. FDA clearances in late 2025 demonstrate regulatory confidence in ML technologies. Applications span radiology subspecialties, imaging modalities, and diagnostic tasks.
Yet challenges remain. Data limitations, validation gaps, and implementation barriers slow progress. The most successful ML medical imaging tools will address genuine clinical needs with rigorous validation evidence, seamless workflow integration, and ongoing performance monitoring.
For healthcare systems considering ML adoption, start with clearly defined clinical problems where algorithmic support could improve outcomes or efficiency. Evaluate vendor claims critically, demanding external validation evidence and implementation support. Engage radiologists, medical physicists, and IT staff in selection and deployment decisions.
For researchers developing new ML algorithms, prioritize diverse training data, rigorous external validation, and metrics aligned with clinical utility. Engage with regulatory authorities early. Design studies that measure impact on patient care, not just algorithmic performance.
The future of medical imaging will integrate human expertise with machine intelligence. Understanding current capabilities, limitations, and best practices positions healthcare organizations and researchers to harness ML’s potential while avoiding common pitfalls. As datasets grow, methods improve, and regulatory pathways mature, ML will increasingly shape how medicine diagnoses, treats, and monitors disease through medical imaging.