Quick Summary: Machine learning is transforming pharmaceutical development by accelerating drug discovery, improving clinical trial design, and enhancing regulatory decision-making. With FDA and EMA establishing common AI principles in 2026, ML models now predict drug interactions, optimize formulations, and identify patient cohorts with unprecedented accuracy—though challenges remain around data quality, model transparency, and the ~8–10% Phase I-to-approval success rate (industry average) that ML aims to improve.
The pharmaceutical industry stands at a crossroads. Drug development traditionally costs over a billion dollars and spans 10–15 years of exhaustive trial and error. Yet despite these massive investments, the overall success rate from Phase I clinical trials to FDA approval is approximately 8–10% on average (with lower rates in high-attrition areas like oncology). This figure comes from aggregated industry analyses across tens of thousands of compounds.
Machine learning offers a fundamentally different approach. By teaching algorithms to recognize patterns across millions of data points, pharmaceutical researchers can make smarter decisions at every stage—from identifying promising molecular structures to predicting which patients will respond to treatment.
And the regulatory landscape just caught up. On 14 January 2026, the EMA and FDA jointly identified ten principles for good artificial intelligence practice across the medicines lifecycle. This marks the first time global regulators have aligned on AI standards for drug development.
But here’s the thing—not all ML applications deliver equal value. Some models excel at predicting drug-target interactions with high accuracy using reinforcement learning. Others struggle to outperform simple baseline approaches when faced with novel compounds.
Understanding Machine Learning in Pharmaceutical Context
Machine learning refers to algorithms that improve their performance through experience rather than explicit programming. In pharma, this means systems that learn to predict drug properties, identify disease patterns, or optimize formulations by analyzing thousands of previous examples.
The FDA defines artificial intelligence (AI) as “a machine-based system that can, for a given set of human-defined objectives, make predictions, recommendations, or decisions influencing real or virtual environments.” These systems perceive data, abstract it into models through automated analysis, and use model inference to formulate actionable options.
Three core ML approaches dominate pharmaceutical applications:
- Supervised learning trains on labeled datasets—molecules tagged with their biological activity, patients categorized by treatment response. Classification models and random forest approaches show strong performance predicting biomarker profiles and analyzing drug treatments.
- Unsupervised learning finds hidden patterns without predefined labels. These algorithms cluster similar compounds, identify patient subgroups, or detect anomalies in manufacturing data that human observers miss.
- Reinforcement learning optimizes sequential decisions through trial and error. Machine learning approaches including reinforcement learning show high accuracy scoring molecular binding functions—learning which chemical modifications improve drug-target interactions.
Real talk: 80% of ML work involves data processing and cleaning, with only 20% devoted to algorithm application. The pharmaceutical industry generates vast data volumes daily—clinical records, genomic sequences, imaging studies, chemical structures. But raw data alone doesn’t enable ML. It requires standardization, validation, and careful curation.
Drug Discovery and Design Applications
Drug discovery begins with identifying molecules that bind therapeutic targets. Traditionally, researchers synthesized and tested thousands of compounds—hoping to find a few promising candidates. Machine learning accelerates this process by predicting which molecular structures will succeed before synthesis.
Target Identification and Validation
Protein-protein interactions govern cellular processes and represent valuable drug targets. Deep learning models achieve high accuracy validating protein-protein interactions using large datasets of confirmed protein pairs.
The model demonstrates strong sensitivity and specificity across validation datasets—identifying which protein interactions drive disease mechanisms and represent druggable opportunities.
Genomic data adds another dimension. Machine learning models show capability to explain significant portions of polygenic variance using single nucleotide polymorphism data. While these specific applications focus on complex traits, similar approaches identify genetic variants linked to drug response and disease susceptibility.
Molecular Structure Prediction
Designing drug molecules requires balancing multiple properties—potency against the target, absorption into the body, minimal side effects, chemical stability. Machine learning models evaluate these trade-offs across vast chemical spaces containing billions of potential compounds.
The SPARROW algorithm represents recent advances in this area. Developed at MIT, it automatically identifies optimal molecules to test as potential medicines from enormous libraries, accounting for the vast number of factors affecting each choice.
Structure-based virtual screening now processes gigascale chemical spaces rapidly. Fast iterative screening approaches narrow billions of candidate molecules to hundreds worth synthesizing, dramatically reducing time and cost in early discovery.
Formulation Development
Once a promising molecule emerges, formulation scientists must determine how to deliver it effectively. Long-acting injectables offer improved efficacy and patient compliance for chronic diseases—but designing these complex polymer-based systems typically requires extensive experimentation.
Machine learning models predict drug release profiles from polymer formulations by analyzing physicochemical properties: molecular weight, polar surface area, heteroatom count, melting temperature, partition coefficient. Training on 80% of drug-polymer combinations and testing on the remaining 20%, these models guide formulation design and reduce development timelines.
The interplay between drug properties and polymer characteristics makes intuitive prediction nearly impossible. ML handles these multidimensional relationships, identifying optimal formulation candidates without exhaustive lab testing.
Clinical Trial Optimization
Clinical trials represent the most expensive and time-consuming phase of drug development. Only 12% of programs succeed from phase 1 to product launch. Patient recruitment consumes substantial portions of development timelines and represents significant costs across the industry.
Phase 3 study planning and patient enrollment timelines span months before testing begins. Machine learning attacks these inefficiencies from multiple angles.
Patient Stratification and Recruitment
Not all patients respond identically to treatment. Genomic variants, disease subtypes, and comorbidities create heterogeneous populations where drugs help some individuals but not others. Traditional trials often mix these groups, diluting positive signals and increasing failure rates.
Machine learning enables precision patient selection. Classification models analyze electronic health records, genetic profiles, and biomarker data to identify individuals most likely to benefit from investigational therapies. This stratification improves trial success rates and accelerates recruitment of appropriate candidates.
High-content phenotypic screening platforms combined with ML identify patient subgroups by cellular response patterns. Companies like Recursion and Janssen apply these approaches to target discovery, hit identification, and toxicity testing—using cell imaging data that traditional analysis largely ignores.
Dose Selection and Safety Monitoring
Determining safe and effective dosing requires balancing therapeutic benefit against adverse effects. ML models predict dose-response relationships from preclinical data, guiding initial human dose selection and subsequent escalation strategies.
During trials, real-time safety monitoring algorithms detect adverse event patterns earlier than conventional methods. These systems flag potential toxicity signals by analyzing accumulating clinical data, enabling faster intervention when problems emerge.
Adaptive trial designs use ML to modify protocols based on interim results—reallocating patients to more promising treatment arms, adjusting doses, or enriching enrollment criteria. This flexibility improves efficiency while maintaining statistical rigor.
Endpoint Prediction and Trial Success
Clinical endpoints determine whether trials succeed or fail. ML models predict primary endpoint achievement using early biomarkers, baseline characteristics, and interim measurements. These predictions help sponsors make go/no-go decisions before investing in lengthy, expensive studies.
Yet challenges remain. Models trained on one disease or population often fail when applied to different contexts. The 90% clinical development failure rate persists despite computational advances—highlighting that ML augments rather than replaces human judgment and rigorous science.
Regulatory Decision Support
On 6 January 2025, the FDA issued draft guidance on using artificial intelligence for drug and biological product development. The draft recommendations address AI systems intended to support regulatory decisions about a product’s safety, effectiveness, or quality.
Commissioner statements emphasized the agency’s commitment to supporting innovative approaches while ensuring rigorous standards. The guidance provides a framework to advance credibility of AI models used throughout the development process.
The FDA-EMA Joint Principles
Following the FDA’s January 2025 guidance, the two agencies jointly identified ten principles for good AI practice on 14 January 2026. These principles span the entire medicines lifecycle—from early research through post-market monitoring.
Key themes include:
- Transparency and explainability: Regulatory reviewers must understand how AI models reach conclusions
- Data quality and representativeness: Training data should reflect diverse populations and use cases
- Validation and performance monitoring: Models require rigorous testing and ongoing surveillance
- Human oversight: AI augments rather than replaces human decision-making
- Ethical considerations: Systems must respect privacy, avoid bias, and promote equitable access
The European Medicines Agency’s reflection paper on AI in the medicinal product lifecycle covers similar territory. It emphasizes principles relevant to applying AI and machine learning at any development step, including manufacturing, pharmacovigilance, and clinical decision support.
Qualification Opinions and Real-World Applications
EMA issues qualification opinions for AI-based tools. A qualification opinion for AI-based measurement of non-alcoholic steatohepatitis histology in liver biopsies was available for public consultation between December 2024 and January 2025—demonstrating regulatory acceptance of validated ML tools for endpoint assessment.
These formal qualifications provide confidence that AI measurements will satisfy regulatory requirements when used in pivotal trials. The process evaluates model performance, data quality, validation methodology, and clinical relevance.
Regulatory reviewers increasingly encounter AI throughout submissions. Software as a Medical Device (SaMD) applications frequently incorporate ML for diagnostic interpretation, treatment recommendations, or patient monitoring. The FDA’s ongoing work on AI/ML-based SaMD establishes principles for these continuously learning systems.

Accelerate Pharma Innovation with Advanced Machine Learning
The pharmaceutical industry is full of complex challenges, including data analysis, R&D optimization, and operational efficiency. AI Superior helps pharma companies harness machine learning to improve decision-making, automate workflows, and derive actionable insights from large datasets.
Unlock Smarter Solutions for Pharma with AI
AI Superior delivers:
- Custom machine learning models for analyzing large pharmaceutical datasets
- Predictive analytics to support research and development strategies
- AI-powered solutions for improving operational workflows and efficiency
👉Contact AI Superior to discuss how machine learning can enhance your pharmaceutical operations and research processes.
Implementation Challenges and Solutions
Despite promising applications, pharmaceutical ML faces substantial obstacles. Understanding these challenges helps organizations implement AI effectively rather than pursuing hype-driven initiatives that fail.
Data Quality and Availability
High-quality data represents the foundation of successful ML. But pharmaceutical data sources are notoriously messy—inconsistent formats, missing values, measurement errors, batch effects, and confounding variables plague datasets.
Remember: 80% of ML work involves cleaning and processing data, with only 20% spent on algorithms. Organizations often underestimate this reality, expecting quick wins from sophisticated models applied to unprepared data.
Small dataset sizes compound the problem. While consumer tech companies train on millions of examples, pharma projects often have hundreds of compounds, dozens of patients, or limited experimental replicates. Few-shot learning approaches show promise for small datasets (under 50 molecules), but performance remains inconsistent.
Data diversity matters as much as quantity. Models trained on narrow chemical spaces or homogeneous patient populations generalize poorly. A 2025 benchmarking study of deep learning models for anticancer drug potency prediction (published 2025-07-01) found all algorithms exhibited sharply reduced accuracy when tested on unseen compounds compared to randomly split training data.
Model Selection and Performance
The “no-free lunch” theorem states no single algorithm outperforms at all possible tasks. Recent research identified a “goldilocks zone” for different ML approaches based on dataset size and diversity:
- Small datasets (under 50 molecules): Few-shot learning models outperform both classical ML and transformers.
- Small-to-medium datasets (50-240 molecules) with high diversity: Transformer models (like MolBART) excel over classical and few-shot approaches.
- Larger datasets with sufficient size: Classical models (support vector regression, random forests) perform best.
This framework helps teams select appropriate algorithms rather than defaulting to the newest architecture. Context matters more than model complexity.
Importantly, several deep learning algorithms could not significantly outperform the Baseline model in many tests. A mean-based baseline—predicting the average value from training data—competed surprisingly well against sophisticated neural networks, especially for unseen compounds.
Interpretability and Trust
Black-box models create friction in pharmaceutical applications where understanding causality matters. Regulators, clinicians, and scientists need explanations—not just predictions.
Techniques like SHAP (SHapley Additive exPlanations) and LIME (Local Interpretable Model-agnostic Explanations) help interpret complex models by showing which features most influenced specific predictions. These methods don’t fully solve interpretability challenges but provide useful insights into model behavior.
Simpler models—decision trees, linear regressions, rule-based systems—offer inherent interpretability at the cost of reduced performance on complex tasks. The trade-off between accuracy and explainability requires careful consideration based on use case stakes and regulatory requirements.
| Challenge | Impact | Solution Approach | Adoption Status |
|---|---|---|---|
| Data quality issues | 80% of ML effort spent on cleaning vs. 20% on algorithms | Standardized data pipelines, automated validation | Widely implemented |
| Small dataset sizes | Models fail on novel compounds; few-shot learning needed | Transfer learning, data augmentation, cross-company sharing | Emerging practices |
| Model interpretability | Regulatory and clinical acceptance requires explainability | SHAP, LIME, simpler model architectures | Partially addressed |
| IC50 variability | 400% variation in potency measurements across protocols | Standardized assays, ensemble predictions | Under development |
| Generalization failure | Sharp accuracy drops on unseen chemical scaffolds | Diverse training sets, scaffold-based splitting | Active research area |
Organizational and Cultural Barriers
Technical challenges pale compared to organizational resistance. Pharmaceutical companies have established workflows, regulatory precedents, and risk-averse cultures that slow AI adoption.
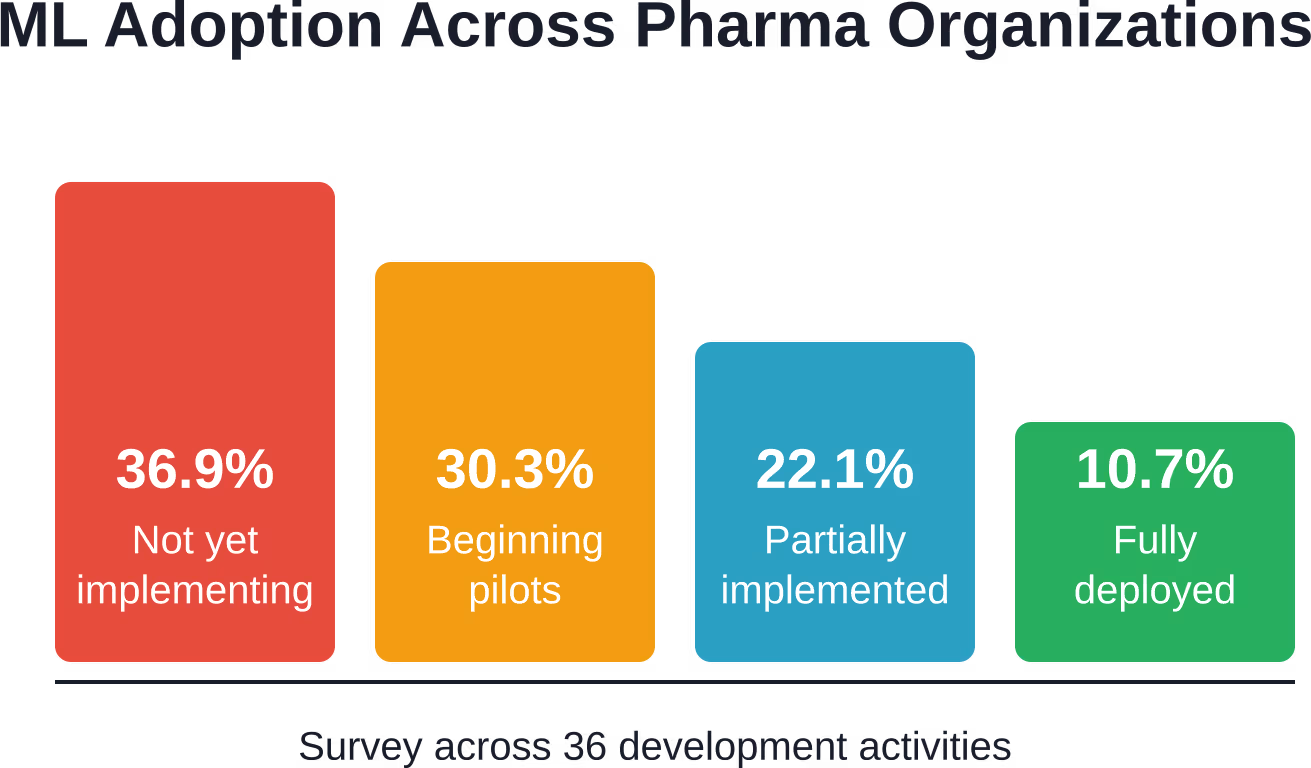
Survey data indicates approximately 36.9% of pharmaceutical organizations had not yet begun using or implementing AI/ML across key development activities. Another 30.3% were just beginning implementation or piloting, 22.1% were partially implementing, and only a minority had advanced beyond pilots.
Successful adoption requires cross-functional collaboration—data scientists working alongside medicinal chemists, clinicians, regulatory experts, and manufacturing specialists. These groups speak different languages, prioritize different metrics, and approach problems from distinct perspectives.
Training programs help bridge these gaps. Organizations need to educate domain experts on ML capabilities and limitations while teaching data scientists pharmaceutical principles. Hybrid roles—individuals with deep expertise in both areas—prove especially valuable but remain scarce.
Real-World Success Stories
Beyond hype and theoretical potential, several organizations have demonstrated measurable ML impact in pharmaceutical settings.
Recursion and High-Content Imaging
Recursion combines high-content phenotypic screening with ML to extract insights from cellular imaging data. Their platform captures millions of cell images under different treatment conditions, then applies deep learning to identify subtle phenotypic changes.
This approach enables target discovery, hit identification, and toxicity prediction by recognizing biological patterns invisible to human observers. Partnerships with major pharmaceutical companies validate the commercial viability of this ML-first strategy.
DeepCDR, DrugCell, and Cancer Drug Prediction
A benchmarking study evaluated five deep learning models for predicting anticancer drug potency (IC50 values): DeepCDR, DrugCell, PaccMann, Precily, and tCNN. Testing used standardized GDSC datasets and recently published anticancer compounds.
Results showed DeepCDR, DrugCell, and tCNN held slight advantages in most scenarios, though all models performed similarly overall. They excelled on randomly split data and unseen cell lines but struggled with novel chemical compounds—highlighting generalization challenges.
Importantly, these sophisticated architectures could not significantly outperform the Baseline model in many tests. This sobering finding underscores that model complexity doesn’t guarantee superior performance.
Assessing prediction error against physicochemical and biological properties of compounds and cell lines revealed weak correlation, highlighting an underexplored aspect of model performance.
Long-Acting Injectable Formulation Design
Researchers applied ML to predict drug release from polymer-based long-acting injectables. These formulations offer improved therapeutic efficacy, safety, and patient compliance for chronic diseases—but designing them traditionally requires extensive experimentation.
The ML models analyzed drug molecular weight, topical polar surface area, heteroatom count, melting temperature, acid dissociation constant, partition coefficient, and corresponding polymer properties. Trained on 80% of formulation data, the models successfully predicted release profiles for the remaining 20%.
This data-driven approach reduces time and cost in formulation development by identifying promising candidates before lab testing. It demonstrates ML’s practical value in pharmaceutical manufacturing—not just discovery research.
Future Directions and Emerging Technologies
Machine learning in pharma continues evolving rapidly. Several trends will shape the next phase of adoption.
Large Language Models and Transformers
Transformer architectures—the foundation of large language models like ChatGPT—now extend beyond natural language to molecular design. MolBART and similar models treat chemical structures as sequences, learning patterns across millions of compounds.
These models excel with small-to-medium datasets (50-240 molecules) that exhibit high diversity. They capture complex structural relationships that classical models miss.
However, transparency concerns remain. A study of AI manuscript generation found the preliminary text obtained directly from ChatGPT showed identical 4.3%, minor changes 13.3%, and related meaning 16.3% compared to the final version after human revision—illustrating that even advanced language models require substantial human oversight.
Multimodal AI Integration
Future systems will integrate diverse data types—chemical structures, genomic sequences, protein structures, cell images, clinical records, literature text. This multimodal approach mirrors how human experts synthesize information from multiple sources.
Early examples combine imaging, omics data, and clinical variables to predict treatment response. As data integration improves, models will capture biological complexity more completely.
Federated Learning and Data Sharing
Small datasets limit pharmaceutical ML progress. But competitive concerns and privacy regulations restrict data sharing between organizations.
Federated learning offers a solution—training models across multiple institutions without centralizing sensitive data. Algorithms learn from distributed datasets while keeping proprietary information secure.
Regulatory initiatives support this direction. The FDA-EMA joint principles emphasize data representativeness and diversity, encouraging collaboration that benefits patients without compromising intellectual property.
Continuous Learning Systems
Traditional ML models are static—trained once, then deployed unchanged. But pharmaceutical knowledge accumulates continuously as new experiments complete, trials report results, and drugs reach the market.
Continuous learning systems update their knowledge automatically as new data arrives. The FDA’s work on Software as a Medical Device with AI/ML capabilities addresses regulatory frameworks for these evolving systems.
Challenges include ensuring updates maintain safety and effectiveness, validating model performance as it changes, and establishing appropriate oversight without stifling innovation.
Practical Implementation Roadmap
Organizations looking to implement pharmaceutical ML should follow a staged approach rather than attempting wholesale transformation.
Phase 1: Foundation Building (Months 1-6)
Start by establishing data infrastructure. Implement standardized data collection, storage, and quality control processes. Remember that 80% of ML work involves data preparation—cutting corners here guarantees failure.
Identify high-value use cases with clear success metrics. Focus on problems where ML offers genuine advantages over existing methods. Avoid applications driven by hype rather than practical need.
Build cross-functional teams combining domain expertise with data science skills. Provide training so scientists understand ML capabilities and limitations while data teams learn pharmaceutical principles.
Phase 2: Pilot Projects (Months 6-18)
Launch targeted pilots addressing specific problems—predicting compound solubility, identifying clinical trial candidates, optimizing manufacturing parameters. Keep initial scope narrow to demonstrate value quickly.
Validate model performance rigorously using appropriate metrics. Don’t rely solely on accuracy—assess calibration, generalization to new examples, performance on edge cases, and comparison to baseline approaches.
Document everything. Regulatory submissions require detailed model development records, validation studies, and performance monitoring plans. Establish these practices during pilots rather than retrofitting later.
Phase 3: Scaled Deployment (Months 18-36)
Expand successful pilots to broader applications. Integrate ML predictions into decision workflows—but maintain human oversight. AI augments expertise; it doesn’t replace judgment.
Implement continuous monitoring of deployed models. Performance can degrade as data distributions shift or new biological mechanisms emerge. Establish processes for detecting problems and updating models.
Engage regulators early when ML will support submissions. The FDA and EMA welcome pre-submission discussions about novel methodologies. Proactive engagement reduces approval risks.
Phase 4: Organizational Transformation (Year 3+)
ML becomes embedded in standard practices rather than special projects. Data-driven decision-making spreads across discovery, development, manufacturing, and post-market surveillance.
Invest in advanced capabilities—federated learning, multimodal models, continuous learning systems. Contribute to industry consortia developing shared resources and standards.
Measure impact quantitatively. Track metrics like development timeline reductions, improved clinical trial success rates, cost savings, and faster time-to-market. Use these metrics to guide ongoing investment.
| Implementation Phase | Timeline | Key Activities | Success Metrics |
|---|---|---|---|
| Foundation Building | 0-6 months | Data infrastructure, team formation, use case selection | Clean datasets, trained staff, approved pilots |
| Pilot Projects | 6-18 months | Targeted ML applications, validation, documentation | Model performance vs. baseline, ROI demonstration |
| Scaled Deployment | 18-36 months | Broader rollout, workflow integration, regulatory engagement | Adoption rates, decision impact, submission readiness |
| Transformation | 3+ years | Cultural shift, advanced capabilities, industry leadership | Timeline reduction, success rate improvement, cost savings |
Ethical Considerations and Responsible AI
Pharmaceutical ML raises important ethical questions that technical performance alone cannot address.
Bias and Health Equity
ML models learn patterns from training data—including biases present in that data. If clinical trials historically underrepresented certain populations, models trained on trial results may perform poorly for those groups.
Genomic models trained predominantly on European ancestry populations show reduced accuracy for other genetic backgrounds. Drug response predictions likewise suffer when training data lacks diversity.
Addressing these issues requires deliberate effort to collect representative data, validate performance across subgroups, and adjust models when disparities emerge. The FDA-EMA principles emphasize data representativeness for precisely these reasons.
Privacy and Data Protection
Pharmaceutical ML requires sensitive data—patient health records, genetic information, treatment outcomes. Protecting privacy while enabling beneficial research creates tension.
Anonymization techniques help but aren’t foolproof. Genomic data in particular can identify individuals even after removing obvious identifiers. Federated learning and differential privacy offer technical solutions, though at some performance cost.
Regulatory frameworks like GDPR and HIPAA establish requirements that pharmaceutical AI must satisfy. Organizations need robust data governance ensuring compliance while enabling innovation.
Transparency and Informed Consent
When ML influences treatment decisions or clinical trial design, affected individuals deserve to know. But explaining complex models to patients and trial participants challenges even experts.
Consent processes should disclose AI involvement without requiring deep technical understanding. Explaining what data the model uses, what it predicts, how predictions inform decisions, and what human oversight exists provides meaningful transparency.
Black-box models complicate this obligation. If developers can’t explain why a model made a specific prediction, obtaining truly informed consent becomes difficult.
Key Takeaways for Pharmaceutical Organizations
So where does this leave pharmaceutical development in 2026?
Machine learning delivers genuine value across drug discovery, clinical trials, and regulatory processes—but not as a silver bullet solving all problems. The ~8–10% approval success rate improves incrementally rather than transforming overnight. ML augments human expertise; it doesn’t replace rigorous science.
Organizations succeeding with pharmaceutical AI share common characteristics:
- They prioritize data quality over model sophistication: Clean, well-curated datasets matter more than the newest architecture. Spending 80% of effort on data preparation isn’t a bug—it’s the reality of effective ML.
- They match models to problems: Few-shot learning for small datasets, transformers for diverse medium datasets, classical methods for large datasets. Context determines optimal approaches.
- They maintain realistic expectations: Deep learning models sometimes can’t beat simple baselines. Understanding when ML adds value versus when traditional methods suffice avoids wasted effort.
- They embrace regulatory engagement: The January 2026 FDA-EMA joint principles provide a roadmap. Following these guidelines from the start prevents costly retrofitting later.
- They build cross-functional teams: Data scientists need pharmaceutical domain knowledge. Scientists need to understand ML capabilities and limitations. Hybrid expertise drives success.
- They address ethical considerations proactively: Bias, privacy, transparency, and equity aren’t afterthoughts—they’re design requirements for responsible AI.
The pharmaceutical industry stands at an inflection point. Machine learning offers genuine opportunities to accelerate development, reduce costs, and improve patient outcomes. But realizing this potential requires moving beyond hype to thoughtful implementation grounded in data quality, appropriate methodology, and regulatory alignment.
Look: technology exists. The regulatory frameworks are emerging. The question now is execution—implementing ML where it delivers real value while avoiding pitfalls that have derailed previous AI waves in healthcare.
Frequently Asked Questions
What is the current success rate for drug development and how does ML improve it?
The overall success rate from Phase I to approval is approximately 8–10% on average. ML-enhanced programs in some cases show higher phase transition success (e.g., approaching or exceeding 12% in targeted applications), though overall rates remain challenging.
Which machine learning approaches work best for different pharmaceutical datasets?
The optimal ML approach depends on dataset size and diversity. Few-shot learning models outperform for small datasets under 50 molecules. Transformer models like MolBART excel with small-to-medium datasets (50-240 molecules) showing high diversity. Classical models such as support vector regression and random forests perform best for larger datasets with sufficient examples. This “goldilocks zone” framework helps teams select appropriate algorithms rather than defaulting to the newest architecture.
What regulatory guidance exists for using AI in drug development?
The FDA issued draft guidance on AI for drug development on 6 January 2025, addressing systems intended to support regulatory decisions about safety, effectiveness, or quality. On 14 January 2026, the FDA and European Medicines Agency jointly identified ten principles for good AI practice across the medicines lifecycle. These principles emphasize transparency, data quality, validation, human oversight, and ethical considerations. The EMA also issues qualification opinions for specific AI tools, such as the AI-based measurement system for non-alcoholic steatohepatitis histology available for public consultation between December 2024 and January 2025.
What are the biggest challenges facing pharmaceutical ML implementation?
Data quality represents the primary challenge—80% of ML effort goes to cleaning and processing versus 20% on algorithms. Small dataset sizes limit model training and generalization. Models show sharp accuracy drops on unseen compounds compared to randomly split training data. IC50 measurements vary by 400% across different assay protocols, creating noise in training data. Organizational barriers also matter: 36.9% of pharmaceutical organizations hadn’t begun AI implementation across key development activities. Cultural resistance, lack of cross-functional expertise, and difficulty demonstrating ROI slow adoption beyond pilot projects.
How accurate are current ML models for drug discovery and development?
Accuracy varies by application. Deep learning models achieve high accuracy validating protein-protein interactions. Machine learning approaches including reinforcement learning reach high accuracy scoring molecular binding functions. Classification models and random forest approaches show strong performance predicting biomarker profiles and analyzing drug treatments. However, benchmarking studies show deep learning models for anticancer drug potency often can’t significantly outperform simple mean-based baseline models, especially for novel compounds. Context matters enormously—reported accuracy on training data or known examples often exceeds real-world performance on new molecules.
What ROI can pharmaceutical companies expect from ML investments?
Quantifying ROI remains challenging due to long development timelines. Key benefits include reduced patient recruitment costs and timelines (which can consume ~30% of trial budgets), faster identification of promising candidates, and improved phase transition success rates.
Machine learning can help lift overall Phase I-to-approval rates from the current industry average of ~8–10%, though gains are incremental rather than dramatic. Focus on measurable metrics: timeline reductions, higher early-phase success, and cost savings in specific processes.
How can smaller pharmaceutical and biotech companies adopt ML without massive resources?
Start with focused applications addressing specific high-value problems rather than attempting comprehensive transformation. Leverage pre-trained models and transfer learning to minimize data requirements. Collaborate through industry consortia and federated learning initiatives that pool knowledge without sharing proprietary data. Use cloud-based ML platforms that eliminate infrastructure investment. Partner with academic institutions and contract research organizations offering ML expertise. Focus initial efforts on data quality and standardization—clean datasets enable effective ML even with simpler models. Consider classical algorithms (support vector machines, random forests) that deliver strong performance on many pharmaceutical tasks without requiring specialized expertise or computational resources that deep learning demands.
Conclusion
Machine learning has moved from theoretical promise to practical reality in pharmaceutical development. The January 2026 FDA-EMA joint principles mark regulatory acceptance of AI across the medicines lifecycle. Success stories demonstrate measurable impact in drug discovery, formulation design, clinical trials, and regulatory submissions.
But challenges remain substantial. Data quality issues, small dataset sizes, model interpretability concerns, and organizational barriers slow adoption. The ~8–10% clinical success rate improves incrementally rather than transforming overnight.
Organizations that succeed will prioritize data infrastructure over algorithm sophistication, match models to problems based on dataset characteristics, maintain realistic expectations about what ML can achieve, engage regulators proactively, build cross-functional expertise, and address ethical considerations from the start.
The pharmaceutical industry has spent decades optimizing traditional approaches. Machine learning offers a fundamentally different path—one that learns from data rather than relying solely on mechanistic understanding. Both approaches have value. The future belongs to organizations that integrate them effectively.
Ready to implement pharmaceutical ML in your organization? Start by assessing your data infrastructure and identifying high-value use cases where predictive modeling addresses real bottlenecks. Build cross-functional teams, launch focused pilots, validate rigorously, and scale what works. The technology is ready. The regulatory frameworks are emerging. The opportunity is now.