Quick Summary: Machine learning in radiology leverages advanced algorithms to analyze medical images, detect abnormalities, and assist radiologists in making faster, more accurate diagnoses. Studies show ML models achieve sensitivity rates between 0.81 to 0.99 for conditions like lung cancer detection, though external validation reveals performance drops of approximately 0.03 AUC points compared to internal testing. FDA-cleared AI tools are already deployed in clinical settings, transforming workflows while raising important questions about generalizability, training data quality, and clinical integration.
Medical imaging generates massive amounts of data every single day. Radiologists face mounting pressure to interpret scans faster without sacrificing accuracy.
Machine learning offers a solution. These algorithms can spot patterns in CT scans, MRIs, and X-rays that human eyes might miss. But the technology isn’t perfect—and understanding both its capabilities and limitations matters for anyone involved in modern healthcare.
Here’s what machine learning actually delivers in radiology right now, backed by research and real-world deployment data.
What Machine Learning Actually Does in Radiology
Machine learning algorithms analyze medical images to identify abnormalities, segment anatomical structures, and classify disease patterns. Unlike traditional software that follows rigid rules, ML models learn from thousands of annotated images.
The technology operates across several categories of diagnostic tasks. Computer-aided detection systems flag suspicious regions for radiologist review. Classification models differentiate between benign and malignant lesions. Segmentation tools outline tumor boundaries for treatment planning.
Deep learning architectures—particularly convolutional neural networks—have become the dominant approach. These networks process images directly without requiring manual feature engineering. The model itself determines which visual patterns correlate with specific diagnoses.
Current Performance Benchmarks
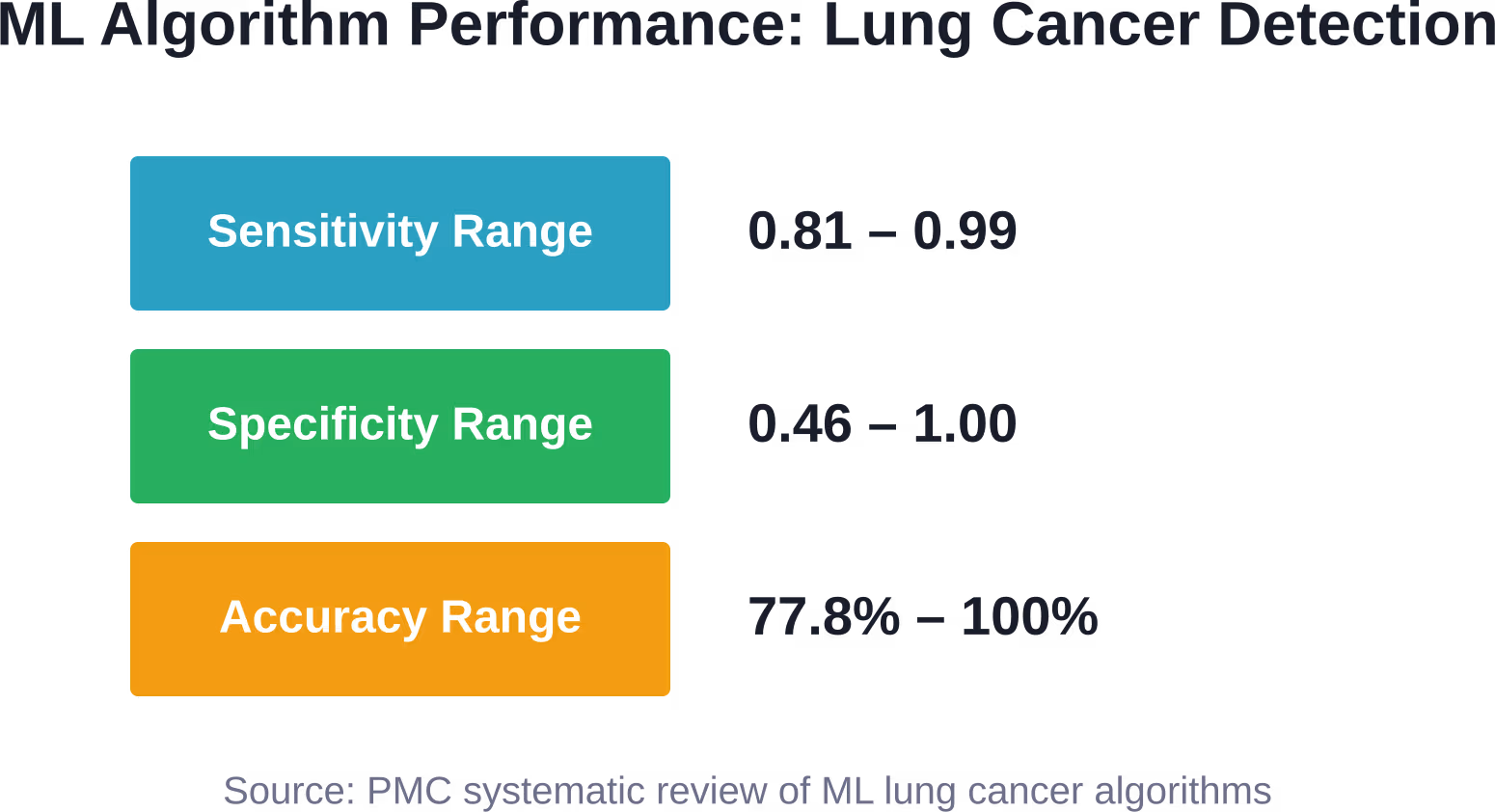
A systematic review analyzing ML algorithms for lung cancer detection found sensitivity ranging from 0.81 to 0.99, with specificity between 0.46 and 1.00. Accuracy spanned 77.8% to 100% depending on the dataset and architecture.
One multi-phase ML architecture achieved 0.97 sensitivity, 0.99 specificity, and 98.0% accuracy for lung lesion analysis. A probabilistic neural network (PNN) architecture reached 0.95 sensitivity, 0.90 specificity, and 92.0% accuracy for lung nodule detection.
But here’s the thing—these numbers come from controlled research settings. Real-world performance often tells a different story.

Develop AI Tools for Medical Image Data With AI Superior
AI Superior builds AI and machine learning solutions, including computer vision, image processing, predictive analytics, NLP, BI, and big data analytics. Their work also includes healthcare-related computer vision projects, such as pill detection and medical image analysis.
For radiology teams, this can support image review, scan analysis, visual classification, reporting support, or decision-support tools built around clinical imaging data.
Need AI Built for Imaging Workflows?
AI Superior can help with:
- building computer vision and ML tools
- analyzing medical image data
- testing ideas through PoC or MVP work
- connecting AI tools with existing systems
👉 Contact AI Superior to discuss your project.
The Generalizability Problem Nobody Talks About
Internal validation makes ML models look impressive. External validation reveals the cracks.
A systematic review examining AI generalizability in radiology identified 342 initial records from PubMed and Embase searches. After screening and eligibility assessment, only 6 studies met the inclusion criteria—a signal that rigorous external validation remains rare.
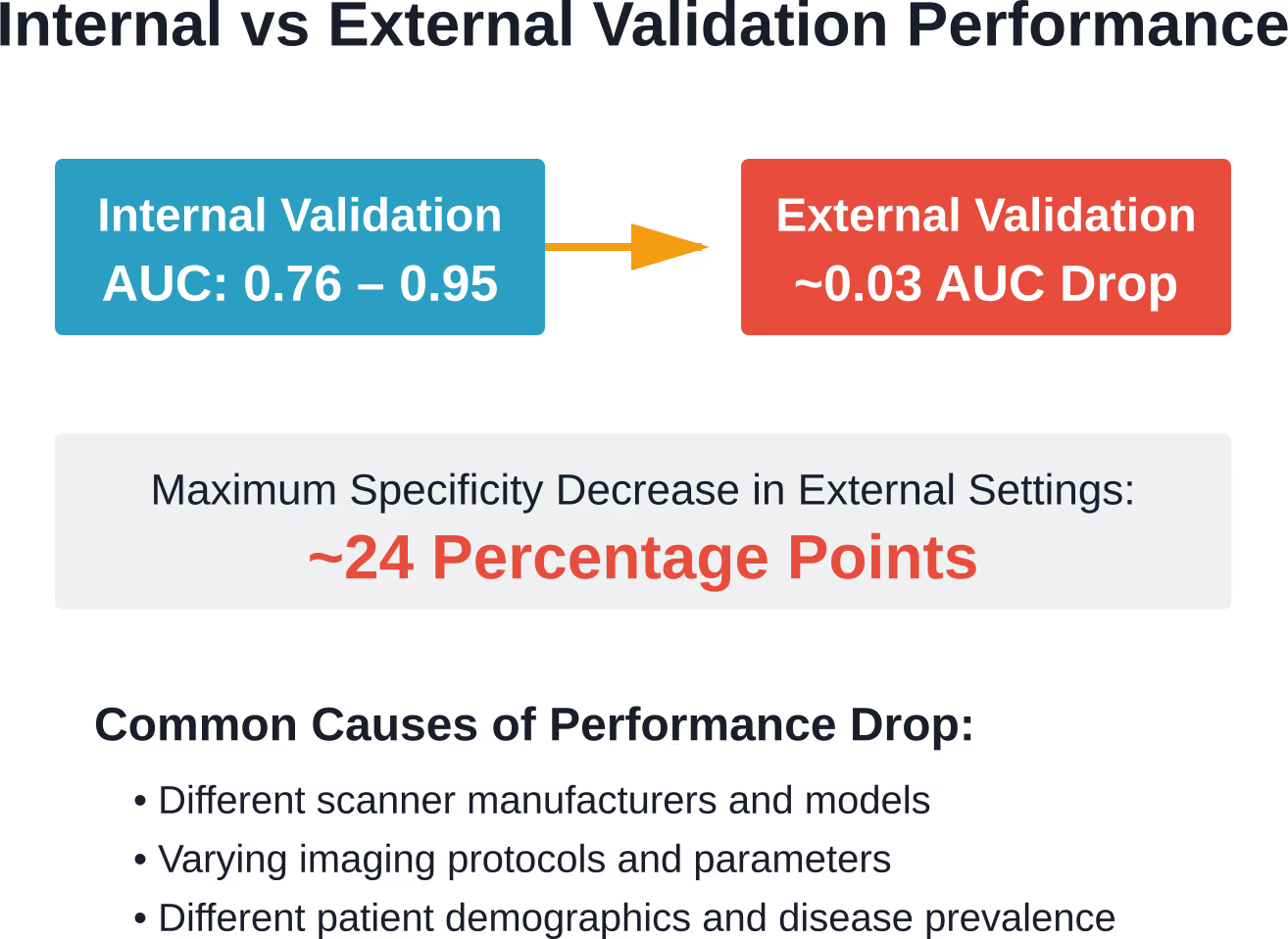
Those six studies used deep learning architectures including 3D convolutional neural networks and generative adversarial networks. Internal validation produced area under curve (AUC) values ranging from 0.76 to 0.95. Sensitivity generally exceeded 85%, and specificity topped 68%.
The drop during external validation? A median AUC decrease of approximately 0.03. Specificity saw maximum decreases around 24 percentage points when models encountered data from different hospitals.
Real talk: models trained on images from one institution often struggle when deployed elsewhere. Scanner types, imaging protocols, patient demographics—all these factors shift between settings. A model that performs brilliantly at an academic medical center might stumble at a rural hospital using different equipment.
Why Models Fail in New Settings
Training data determines everything. Models learn the specific characteristics of images in their training set—including quirks that don’t generalize.
Different scanners produce different noise patterns. Imaging protocols vary between institutions. Patient populations differ demographically and clinically. A model trained predominantly on one ethnic group may perform worse on others. Geographic variation in disease prevalence affects positive predictive value.
Data annotation introduces another variable. Multiphase reviews and expert adjudication improve label quality, but many datasets rely on single-reader annotations or majority voting. Ambiguous cases get mislabeled. Models learn incorrect patterns.
Clinical Applications Already Deployed
The FDA maintains a list of AI-enabled medical devices authorized for marketing in the United States. Recent clearances include imaging systems and diagnostic tools already in clinical use.
Recent FDA clearances include AI-powered imaging tools. The FDA maintains an AI-Enabled Medical Device List of authorized products currently deployed in clinical settings. These represent just the latest additions to a growing ecosystem.
Computer-aided detection for pulmonary embolism represents one established application. One PE CAD system reported 80% sensitivity at 4 false positives per patient on a CTA dataset of 177 cases. The system uses multiple-instance classification to reduce false positives before making final diagnoses.
Anterior Cruciate Ligament Injury Detection
Anterior cruciate ligament (ACL) injury is a common sports injury with significant clinical impact. Machine learning systems trained on MRI images aim to improve diagnostic accuracy and reduce interpretation time. ACL injuries carry significant healthcare costs associated with treatment and reconstruction surgery.
Machine learning systems trained on MRI images aim to improve diagnostic accuracy and reduce interpretation time. Early detection enables better treatment planning and potentially better outcomes.
The models analyze ligament structure, signal intensity, and surrounding tissue patterns. Some architectures achieve performance comparable to experienced musculoskeletal radiologists on internal validation sets.
Deep Learning Architectures Dominate Current Research
Convolutional neural networks have become the standard architecture for radiology imaging tasks. These networks process pixel data through layers of learned filters, building increasingly abstract representations.
Early layers detect edges and basic shapes. Middle layers recognize anatomical structures. Deep layers identify complex patterns associated with specific pathologies.
The approach eliminates manual feature engineering. Traditional machine learning required experts to define relevant image characteristics—texture measures, shape descriptors, intensity distributions. CNNs learn these features automatically from training data.
3D convolutional architectures process volumetric imaging data like CT and MRI scans. Standard 2D CNNs analyze individual slices, potentially missing three-dimensional context. 3D networks capture spatial relationships across the entire volume.
Generative Adversarial Networks in Imaging
GANs consist of two competing networks. A generator creates synthetic images. A discriminator tries to distinguish real from synthetic. The generator improves by fooling the discriminator.
In radiology, GANs augment training datasets by generating realistic synthetic images. This addresses the perennial problem of insufficient training data, particularly for rare conditions.
GANs also enhance image quality. Low-dose CT reconstruction uses generative models to reduce noise while preserving diagnostic information. MRI acceleration techniques employ GANs to reconstruct full images from undersampled acquisitions, reducing scan times.
The Data Annotation Bottleneck
Machine learning models need labeled examples. Lots of them. For supervised learning in radiology, that means expert annotations—expensive and time-consuming to obtain.
A single radiologist reviewing images for labeling introduces variability and potential errors. Multiple independent readers improve reliability but multiply the cost. Majority voting helps but can miss challenging cases where expert disagreement signals genuine diagnostic difficulty.
Research shows that adjudication improves consensus among radiologists. When readers disagree, a senior expert reviews the case and provides the authoritative label. This approach creates higher-quality training data than simple majority voting.
Multiphase review processes further enhance label quality. Initial screening identifies clear-cut cases. Subsequent rounds focus on ambiguous findings, applying more rigorous criteria and involving more experienced readers.
The Asymmetric Cost Problem
False positives and false negatives carry different consequences. Missing a malignant lesion (false negative) can delay life-saving treatment. Flagging a benign finding as suspicious (false positive) triggers unnecessary biopsies, patient anxiety, and healthcare costs.
Model training typically treats all errors equally. Adjusting decision thresholds shifts the balance—higher thresholds reduce false positives but increase false negatives, and vice versa.
Clinical deployment requires explicit choices about acceptable trade-offs. Screening applications often prioritize sensitivity, accepting more false positives to minimize missed cancers. Confirmatory testing might emphasize specificity to avoid unnecessary interventions.
Real-World Deployment Challenges
Getting a model to work in research is one thing. Integrating it into clinical workflows is another entirely.
PACS integration represents the first hurdle. Picture Archiving and Communication Systems manage medical imaging across healthcare institutions. AI tools must plug into existing PACS infrastructure without disrupting radiologist workflows.
Output presentation matters enormously. A model that highlights suspicious regions on the image itself provides more actionable information than a simple probability score. Radiologists need to understand what the algorithm detected and why.
Model decay poses an ongoing challenge. Performance degrades over time as imaging equipment gets upgraded, protocols change, and patient populations shift. Continuous monitoring detects performance drops before they impact patient care.
| Deployment Challenge | Impact | Mitigation Strategy |
|---|---|---|
| PACS Integration | Workflow disruption if poorly implemented | Standards-based interfaces, pilot testing |
| Model Decay | Performance degradation over months/years | Continuous monitoring, periodic retraining |
| Explainability | Radiologist distrust without interpretability | Attention maps, saliency visualization |
| Regulatory Compliance | Legal liability, FDA requirements | Clinical validation studies, quality systems |
| Data Privacy | HIPAA violations, patient trust issues | De-identification, secure infrastructure |
The ACR Quality Assurance Framework
The American College of Radiology launched ARCH-AI, the first national artificial intelligence quality assurance program for radiology facilities. The ACR Recognized Center for Healthcare-AI sets guidelines for AI use in imaging interpretation.
The program ensures radiology facilities use AI safely and effectively. It defines best practices for AI deployment, validation, and monitoring in clinical settings.
ACR-SIIM practice parameters outline operational requirements. Qualified personnel include physicians, medical physicists, and radiologic technologists with specific AI competencies. Technical standards address data management, security, and quality control.
Comparing ML Performance to ChatGPT on Radiology Images
How do general-purpose AI models perform on specialized medical imaging tasks? Not great, according to research testing ChatGPT on radiology image analysis.
When tested on radiology image analysis, ChatGPT achieved a 0.61 average diagnostic score, with performance varying significantly by imaging modality. Performance varied by imaging modality. Chest radiographs scored 0.70 on average. Skeletal system images dropped to 0.52.
Partially correct answers accounted for 40% of responses. ChatGPT often provided multiple answer options, with one turning out correct. This suggests the model lacks the focused training required for reliable diagnostic interpretation.
The comparison highlights why specialized models matter. General-purpose language models can’t replace task-specific architectures trained on hundreds of thousands of annotated medical images.
Regulatory Landscape and FDA Clearance
The FDA regulates AI-enabled medical devices as Software as a Medical Device (SaMD). Manufacturers must demonstrate safety and effectiveness before marketing in the United States.
The FDA maintains an AI-Enabled Medical Device List identifying authorized products. The list helps digital health innovators understand the current device landscape and regulatory expectations.
Regulatory evaluation increasingly addresses AI-specific challenges. Locked algorithms follow traditional regulatory pathways. Continuously learning systems that update based on new data require novel assessment paradigms to ensure ongoing safety.
Explainability and Radiologist Trust
Black-box models make radiologists uncomfortable. When an algorithm flags a region without explaining why, trust erodes.
Attention maps and saliency visualization help. These techniques highlight which image regions most influenced the model’s decision. A heat map overlay shows where the network focused its analysis.
But visualization isn’t explanation. Knowing which pixels mattered doesn’t reveal what patterns the model detected or how they relate to pathology.
Clinical validation builds trust through demonstrated performance. When radiologists see a model consistently catching findings they might have missed, confidence grows. When the model generates frequent false alarms on obvious benign cases, skepticism increases.
Fairness and Bias Considerations
Training data demographics determine model fairness. A model trained predominantly on images from one ethnic group may underperform on others.
Gender representation affects performance. Age distribution matters. Geographic variation in disease prevalence influences positive predictive value when models deploy in different populations.
Auditing for bias requires testing on diverse datasets that reflect the intended deployment population. Performance metrics should be stratified by demographic groups to identify disparities.
The Workflow Integration Reality
AI tools don’t replace radiologists. They augment workflows—when implemented thoughtfully.
Triage applications prioritize worklists, moving critical findings to the front of the queue. Time-sensitive conditions like intracranial hemorrhage or pulmonary embolism get flagged for immediate attention.
Second-reader systems provide a safety net. After the radiologist completes their interpretation, the AI reviews the same images. Discrepancies trigger a second look. This catches errors before reports get finalized.
Protocol optimization represents another application. AI assistants analyze requisition information and suggest appropriate imaging protocols, reducing protocol selection errors and streamlining technologist workflows.
| Application Type | Primary Function | Workflow Position |
|---|---|---|
| Triage | Prioritize critical findings | Pre-interpretation |
| Detection Aid | Highlight suspicious regions | During interpretation |
| Second Reader | Quality assurance check | Post-interpretation |
| Protocol Assistant | Optimize scan parameters | Pre-acquisition |
| Quantification Tool | Measure lesion size/volume | During/post interpretation |
Training Data Quantity Requirements
How many labeled images does a model need? The answer depends on task complexity and architectural choices.
Simple binary classification with clear visual differences might work with thousands of examples. Complex multi-class problems with subtle distinctions require tens of thousands or more.
Transfer learning reduces data requirements. Models pre-trained on large natural image datasets (ImageNet, for example) learn general visual features. Fine-tuning on medical images adapts these features to radiology tasks with fewer examples.
Data augmentation artificially expands training sets. Rotating, flipping, scaling, and adjusting image contrast creates variations of existing examples. The model sees more diversity without requiring additional annotations.
Common Failure Modes in Clinical Deployment
Models fail in predictable ways when assumptions break down.
- Distribution shift occurs when deployment data differs systematically from training data. A model trained on chest X-rays from adults struggles with pediatric images. Scanner upgrades change image characteristics. Protocol modifications alter visual appearance.
- Adversarial examples represent deliberate or accidental perturbations that fool models. Small changes imperceptible to humans cause confident misclassifications. Medical imaging faces lower adversarial risk than some domains, but the possibility exists.
- Edge cases expose brittleness. Unusual patient anatomy, rare pathologies, or imaging artifacts not represented in training data generate unpredictable outputs.
- Continuous monitoring detects these failure modes through performance metrics tracked over time. Sudden drops in sensitivity or specificity signal problems requiring investigation.
The Economics of AI in Radiology
Implementing AI involves upfront costs and ongoing expenses. Software licensing fees vary by vendor and deployment scale. Some charge per study, others per radiologist or per facility.
Hardware requirements depend on deployment model. Cloud-based solutions shift compute costs to operating expenses. On-premise deployments require GPU servers and IT infrastructure.
Integration labor shouldn’t be underestimated. PACS interfaces need configuration. Workflow adaptations require planning and training. Technical support costs continue throughout deployment.
The value proposition centers on efficiency gains and quality improvements. Faster turnaround times increase throughput. Reduced error rates decrease downstream costs from missed diagnoses. Whether the math works depends on specific institutional contexts.
Future Directions and Research Frontiers
Multimodal learning combines imaging with clinical data. Models that integrate radiology images, lab results, patient history, and genomic information may outperform image-only approaches.
Federated learning enables training on distributed datasets without centralizing patient data. Institutions collaborate on model development while data remains behind their firewalls. This addresses privacy concerns and enables learning from larger, more diverse populations.
Self-supervised learning reduces annotation requirements. Models learn representations from unlabeled images through pretext tasks, then fine-tune on smaller labeled datasets for specific diagnostic objectives.
Look, the technology keeps evolving. What works today will be outdated in two years. Staying current requires ongoing education and willingness to reassess assumptions.
Frequently Asked Questions
How accurate are machine learning models compared to radiologists?
ML models achieve sensitivity between 0.81 to 0.99 for lung cancer detection, with accuracy ranging from 77.8% to 100% depending on the architecture and dataset. However, these metrics come from controlled research settings. External validation shows performance drops of approximately 0.03 AUC points when models encounter data from different institutions. Models work best as decision support tools alongside radiologists rather than replacements.
What causes AI model performance to drop in different hospitals?
Performance degradation stems from differences in scanner manufacturers, imaging protocols, patient demographics, and disease prevalence. Models learn patterns specific to their training data, including institution-specific quirks. When deployed elsewhere, these learned patterns may not apply. Maximum specificity decreases can reach 24 percentage points in external validation compared to internal testing.
Are FDA-cleared AI radiology tools already available?
Yes. The FDA maintains an AI-Enabled Medical Device List of authorized products. Recent clearances include AIR Recon DL by GE Medical Systems (cleared December 23, 2025) and TruSPECT Processing Station (cleared December 30, 2025). These tools assist with image reconstruction, protocol optimization, and diagnostic detection across various imaging modalities.
How much training data do radiology AI models need?
Requirements vary by task complexity. Simple binary classification might work with thousands of labeled examples, while complex multi-class problems need tens of thousands or more. Transfer learning from models pre-trained on natural images reduces these requirements. Data augmentation techniques—rotating, scaling, and adjusting images—artificially expand training sets without additional manual annotations.
What role does the American College of Radiology play in AI quality?
The ACR launched ARCH-AI, the first national AI quality assurance program for radiology facilities. It sets guidelines for safe and effective AI use in imaging interpretation. ACR-SIIM practice parameters define operational requirements, personnel qualifications, and technical standards for AI deployment in clinical settings. The program helps institutions implement AI while maintaining quality and safety standards.
How do hospitals monitor AI performance after deployment?
Continuous monitoring tracks sensitivity, specificity, and other performance metrics over time. Sudden drops signal problems like model decay, distribution shift, or equipment changes. Institutions implement quality control processes comparing AI outputs against radiologist interpretations on sample cases. When performance degrades, models require retraining on updated data reflecting current equipment, protocols, and patient populations.
Making Informed Decisions About ML in Radiology
Machine learning delivers real value in radiology when deployed thoughtfully. The technology excels at pattern recognition tasks with abundant training data and clear diagnostic criteria.
But it’s not magic. Models reflect their training data—biases, gaps, and all. External validation matters more than impressive internal metrics. Integration challenges extend beyond technical specifications into workflow design and change management.
Radiologists remain central. AI augments human expertise rather than replacing it. The most successful implementations position algorithms as decision support tools that enhance rather than automate clinical judgment.
For institutions considering AI adoption, start with well-defined problems where ML demonstrably adds value. Prioritize vendors offering transparent validation data and robust post-deployment monitoring. Invest in integration and training as seriously as the software itself.
The technology will keep advancing. Performance will improve. New applications will emerge. Staying effective means continuous learning, critical evaluation of vendor claims, and willingness to adapt as evidence accumulates.
Machine learning in radiology isn’t future speculation—it’s current reality. Understanding both capabilities and limitations enables informed decisions that improve patient care while managing realistic expectations.