Quick Summary: Machine learning is revolutionizing pharmaceutical marketing by enabling data-driven personalization, predictive analytics, and real-time physician engagement optimization. The technology analyzes vast datasets to identify physician prescribing patterns, predict patient needs, and deliver precision-targeted messaging that drives measurably better outcomes than traditional approaches.
The pharmaceutical industry stands at a crossroads. Traditional marketing approaches—mass email campaigns, standardized sales rep visits, blanket advertising—are yielding diminishing returns. Physicians receive hundreds of promotional messages weekly, and patients face information overload.
Machine learning changes the equation entirely.
Instead of guessing which message resonates with which physician, ML algorithms analyze prescribing patterns, patient demographics, treatment outcomes, and engagement histories to predict precisely when and how to reach each healthcare provider. The result? Marketing that feels less like promotion and more like valuable clinical intelligence.
But here’s the thing: this isn’t just theory anymore. Pharmaceutical companies report improvements in engagement metrics and sales productivity through machine learning deployment, though specific uplift percentages vary by implementation and context. The technology has matured beyond proof-of-concept into production-grade systems handling billions of data points daily.
This guide breaks down exactly how machine learning reshapes pharma marketing—from the algorithms predicting physician behavior to the regulatory frameworks governing their use. No fluff, no generic AI hype. Just the practical systems, verified outcomes, and strategic frameworks that define best-in-class pharmaceutical marketing in 2026.
The Economic Imperative Driving ML Adoption
Real talk: pharmaceutical companies didn’t embrace machine learning because it sounded innovative. They adopted it because traditional marketing stopped working at scale.
According to research, on average it takes 10–13 years to bring a drug to market, with development costs ranging from $1–2.3 billion. Even more striking? Return-on-investment in pharma plummeted from 10.1% in 2010 to just 1.8% in 2019.
Those economics create immense pressure on every downstream function, including marketing. When development costs spiral, the commercial organization must extract maximum value from launch windows and patent exclusivity periods. There’s zero room for wasted marketing spend or misallocated sales resources.
Machine learning addresses this pressure directly by transforming marketing from an art into a science. Instead of allocating sales rep time equally across territories or running identical campaigns to all specialists, ML systems identify the physicians most likely to prescribe, the messaging most likely to convert, and the timing most likely to drive action.
The precision matters enormously. If traditional approaches convert 2-3% of targeted physicians into prescribers, and ML-optimized targeting converts 5-6%, that difference compounds across thousands of physicians and millions in revenue.
The Data Lag Problem
But there’s a catch that makes pharma marketing uniquely challenging: data lag.
Unlike consumer marketing where purchase behavior updates in real-time, pharmaceutical prescription data typically lags by weeks or months. A physician writes a prescription today, but that data point might not reach the pharmaceutical company’s analytics systems for 4-8 weeks depending on data provider refresh cycles.
This lag creates blind spots. Marketing teams make decisions based on outdated snapshots, unaware that a physician’s prescribing patterns shifted three weeks ago. Campaign optimization happens in slow motion.
Machine learning mitigates this through predictive modeling. Rather than waiting for prescription data, ML algorithms analyze leading indicators—physician engagement patterns, patient demographic shifts, competitive product launches, formulary changes, peer influence networks—to predict prescribing behavior changes before they show up in lagged datasets.
The shift from reactive analysis to predictive intelligence represents the fundamental value proposition of ML in pharma marketing. It’s not about processing data faster; it’s about seeing what’s coming before it arrives.
Core ML Applications Transforming Pharma Marketing
Machine learning in pharmaceutical marketing isn’t a single technology but rather a collection of specialized applications, each addressing specific operational challenges. Here’s where the technology delivers measurable impact.
Physician Targeting and Segmentation
Traditional physician segmentation relied on crude proxies: specialty, geography, prescription volume. Everyone treating condition X in region Y received identical outreach.
Machine learning segments physicians across dozens of behavioral dimensions simultaneously. Algorithms analyze prescribing patterns, treatment protocol preferences, responsiveness to different message types, engagement channel preferences, peer influence networks, patient population characteristics, and historical conversion data.
The result? Micro-segments of 10-50 physicians who share behavioral signatures rather than demographic checkboxes. One segment might consist of early-adopting cardiologists in academic centers who respond to peer-reviewed evidence and prefer digital engagement. Another might be community-based endocrinologists who rely on sales rep relationships and prefer case study formats.
Marketing content, messaging, and channel allocation get customized to each micro-segment’s preferences. Instead of one campaign, the system orchestrates hundreds of variant campaigns, each optimized for a specific behavioral cluster.
This granularity was impossible before machine learning. The combinatorial complexity of matching thousands of physicians to dozens of message variants across multiple channels exceeded human analytical capacity. ML systems handle it routinely.
Predictive Lead Scoring and Next-Best-Action
Sales teams face a resource allocation nightmare: which physicians deserve in-person visits, which respond better to digital outreach, and which aren’t worth contacting at all given current priorities?
Machine learning generates real-time lead scores for every physician in the target universe. These scores synthesize hundreds of signals: recent prescription changes, website engagement, email opens, conference attendance, peer interactions, patient demographic shifts, formulary status updates, and competitive activity.
More powerfully, ML systems recommend next-best-actions for each physician. Not just “this doctor is a high-priority lead” but “this doctor is likely to respond positively to a peer-to-peer discussion about the latest outcomes data, scheduled for late afternoon, following up on the case study they downloaded last week.”
The specificity transforms sales productivity. Reps spend time on physicians genuinely ready to engage, with conversation starters grounded in actual behavioral signals. Conversion rates climb while call volume requirements drop.
Content Personalization at Scale
Pharmaceutical marketing involves enormous content libraries: clinical studies, mechanism-of-action videos, dosing guidelines, safety information, patient case studies, economic analyses, formulary positioning documents, and competitive comparisons.
Which pieces resonate with which physicians? Machine learning recommendation engines answer this by analyzing content consumption patterns, engagement signals, and subsequent prescribing behavior.
When a physician logs into a pharmaceutical company’s medical information portal, the ML system surfaces the 3-5 content pieces most likely to influence their prescribing decisions based on their specialty, practice patterns, recent searches, and behavioral similarity to other physicians who converted after consuming similar content.
This personalization extends across email, websites, sales rep materials, and speaker programs. Every touchpoint adapts to the individual physician’s informational needs and preferences.
The underlying technology borrows from consumer recommendation systems—collaborative filtering, content-based filtering, hybrid models—but adapted for the pharmaceutical industry’s unique constraints around regulatory compliance and evidence-based messaging.
Campaign Performance Optimization
Traditional campaign optimization followed monthly cycles: launch campaign, wait four weeks, analyze results, adjust messaging, relaunch. By the time adjustments took effect, market conditions had shifted.
Machine learning enables continuous optimization. Algorithms monitor campaign performance metrics—open rates, click-throughs, engagement duration, content downloads, follow-up actions—across hundreds of micro-segments simultaneously, adjusting message variants, send times, channel mix, and content recommendations in real-time.
Underperforming message variants get automatically retired. High-performing variants get increased distribution. The system tests new variants continuously, allocating small portions of traffic to experimental messages while the bulk flows to proven winners.
This approach borrows from digital advertising’s programmatic optimization but adapted for pharmaceutical marketing’s longer conversion cycles and regulatory constraints. The system can’t simply maximize clicks; it must balance engagement with compliance, ensuring every optimized variant meets promotional review standards.

Apply ML to Pharma Marketing With AI Superior
Pharma marketing often involves complex data, strict workflows, and careful decision-making. AI Superior can help teams explore machine learning use cases in a structured way, especially when the project involves segmentation, forecasting, content analysis, or internal decision-support tools.
Their services include AI consulting, machine learning, data science, NLP, AI software development, proof of concept development, and model evaluation. This fits pharma marketing projects where the model needs to be tested carefully before it is used in business workflows.
AI Superior can help with:
- Defining a suitable pharma marketing AI use case
- Reviewing structured business, market, or engagement data
- Building proof of concept models
- Developing models for segmentation, forecasting, or text analysis
- Evaluating model quality and reliability
- Planning integration with internal systems or reporting tools
- Supporting AI software development after validation
For pharma marketing, this may be relevant for market segmentation, HCP engagement analysis, campaign performance prediction, content classification, and demand-related forecasting.
Contact AI Superior to discuss the project.
Real-World Data Integration and Analysis
Machine learning’s power in pharma marketing scales directly with data quality and breadth. The most sophisticated implementations integrate multiple real-world data sources into unified physician and patient profiles.
Key Data Sources
Prescription data remains foundational—longitudinal records of which physicians prescribe which medications, at what volumes, to which patient populations, with what treatment outcomes. This data typically comes from pharmacy claims, electronic health records, and specialty pharmacy networks.
But ML systems layer in behavioral data: email engagement, website visits, content consumption, sales rep interaction histories, call center inquiries, conference attendance, peer-to-peer communication patterns, and social media engagement.
Patient-level data adds another dimension: demographics, comorbidities, treatment histories, adherence patterns, outcomes data, and healthcare utilization. Privacy regulations constrain direct use, but aggregated and de-identified patient data informs physician-level analytics—understanding which physicians treat which patient populations helps predict future prescribing needs.
External data enriches the picture further: formulary status updates, payer policy changes, competitive product launches, clinical guideline revisions, regulatory actions, and peer-influenced prescribing networks derived from referral patterns and co-authorship graphs.
The Data Standardization Challenge
Here’s where it gets messy. These data sources use incompatible formats, coding systems, and identifier schemes. Prescription data uses NDC codes; clinical data uses ICD-10; payer data uses formulary-specific codes. Physician identifiers—NPI numbers, DEA numbers, state license numbers—don’t always map cleanly across datasets.
Machine learning helps here too, particularly natural language processing algorithms that standardize free-text fields and probabilistic matching algorithms that link records across systems despite inconsistent identifiers.
Machine learning approaches to data mapping can significantly reduce data integration time compared to manual approaches. That acceleration matters enormously when marketing teams need to integrate a new data source in weeks rather than quarters.
Regulatory and Compliance Frameworks
Machine learning in pharma marketing operates within one of the most stringent regulatory environments in commercial software. Every algorithm, every data integration, every automated decision must align with FDA guidance, HIPAA requirements, PhRMA codes, and international pharmaceutical marketing standards.
The FDA has been actively developing frameworks for AI and machine learning in pharmaceutical contexts. In January 2025, the agency issued draft guidance on the use of artificial intelligence intended to support regulatory decisions about drug and biological product safety, effectiveness, and quality.
While that guidance focuses primarily on drug development rather than marketing, it establishes important principles: transparency in algorithmic decision-making, validation of ML model accuracy, monitoring for bias and drift, and documentation of training data provenance.
Pharmaceutical companies applying ML to marketing adopt similar rigor. Models undergo validation against holdout datasets. Algorithmic recommendations get reviewed by compliance teams before deployment. Audit trails document every automated decision. Bias testing ensures models don’t discriminate based on protected characteristics or create inappropriate prescribing incentives.
The Off-Label Promotion Minefield
One particularly sensitive area: ensuring ML systems don’t inadvertently generate off-label promotional content.
Machine learning models trained on broad medical literature might learn associations between a drug and indications not covered by FDA approval. A content recommendation engine might suggest an article about off-label use to a physician. A chatbot might respond to an off-label question with information that crosses the line into promotion.
Preventing this requires explicit constraints in model training, content filtering layers, and continuous monitoring for edge cases. The most mature implementations employ separate ML models trained specifically to detect potential off-label content before it reaches physicians.
These safeguards add complexity but they’re non-negotiable. A single off-label promotion incident can trigger federal investigations, consent decrees, and nine-figure settlements.
| Regulatory Area | Key Requirement | ML Implementation Challenge | Common Solution |
|---|---|---|---|
| FDA Promotional Review | All promotional materials must be pre-approved | ML generates dynamic personalized content | Template-based generation with pre-approved modules; human review of variants |
| Off-Label Compliance | No promotion for unapproved indications | Models may learn off-label associations from medical literature | Content filtering layers; specialized detection models; restricted training data |
| HIPAA Privacy | Protected health information must be secured | ML models require patient-level data for insights | De-identification; aggregation; differential privacy techniques |
| Adverse Event Reporting | Must report safety signals within specified timeframes | ML may detect signals in unstructured physician feedback | Automated signal detection with pharmacovigilance workflow integration |
| Fair Balance | Risk information must accompany efficacy claims | Personalized messaging might emphasize benefits | Algorithmic fair balance checks; mandatory risk inclusion rules |
Clinical Trial Optimization Through ML
While this guide focuses on marketing, it’s worth noting that machine learning’s impact on clinical trials directly affects downstream marketing operations. Faster, more efficient trials mean earlier launches and longer effective patent life.
Standard industry benchmarks indicate that Phase 1 trials average approximately 22 months, Phase 2 average 29 months, and Phase 3 average 40 months.
Machine learning optimizes multiple aspects of trial execution: patient recruitment and eligibility screening, site selection based on enrollment potential, adaptive trial design that adjusts based on interim results, and predictive modeling of trial outcomes.
For marketing teams, these improvements mean more reliable launch timelines and better market access planning. When ML models predict with 80-85% accuracy which trials will meet endpoints, commercial organizations can invest confidently in pre-launch marketing preparation.
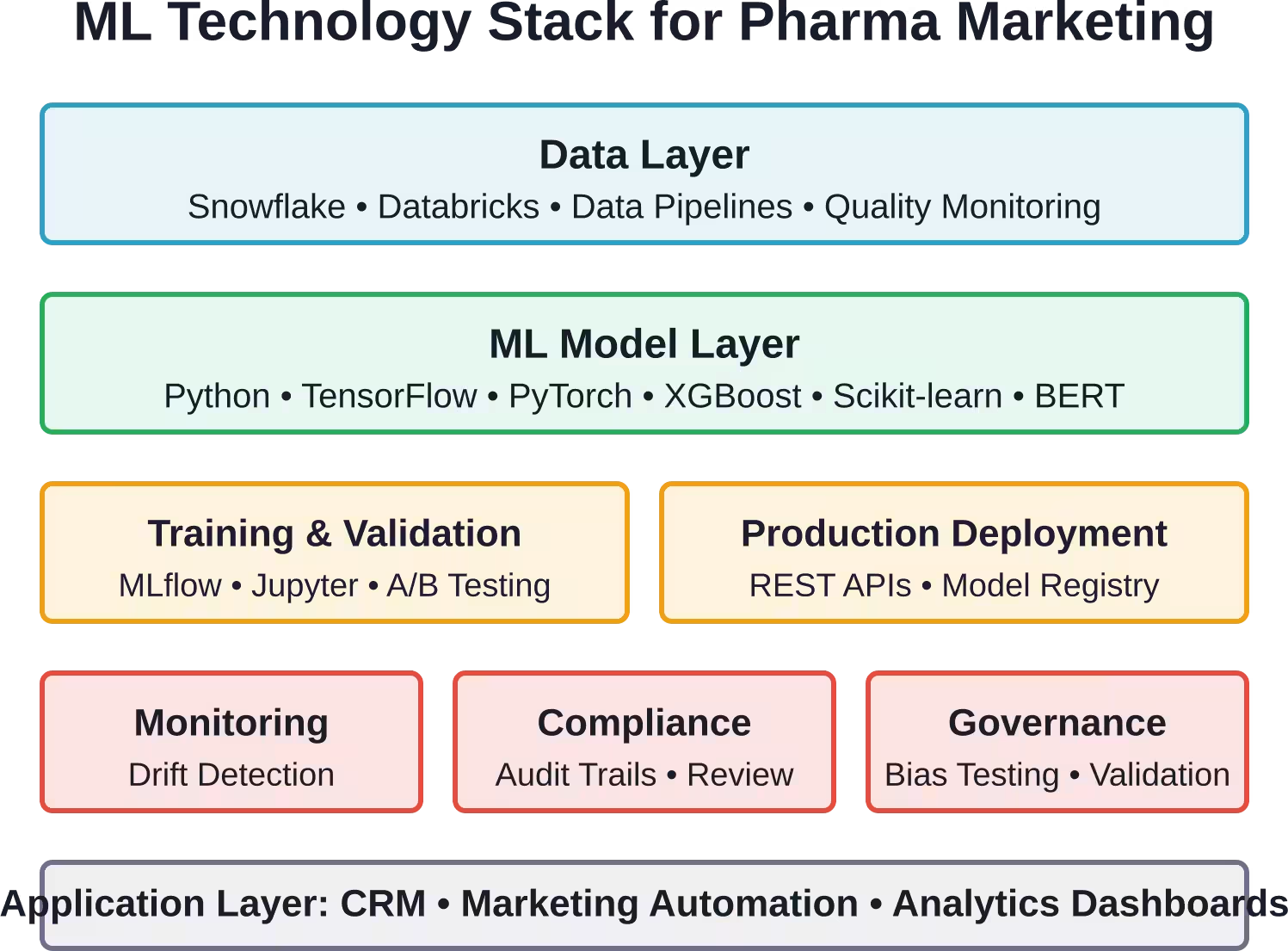
Implementation Architecture and Technology Stack
Building production-grade machine learning for pharma marketing requires specific architectural patterns and technology choices. Here’s what best-in-class implementations look like under the hood.
Data Infrastructure
The foundation is a unified data warehouse integrating prescription data, behavioral data, patient data, and external intelligence. Most implementations use cloud-based data platforms—Snowflake, Databricks, or Google BigQuery—capable of handling billions of rows and complex joins across dozens of source systems.
Data pipelines run continuously, ingesting new prescription files, engagement events, and third-party feeds. Streaming pipelines handle real-time behavioral data—website clicks, email opens, CRM updates—while batch pipelines process larger datasets on daily or weekly schedules.
Data quality monitoring runs in parallel, flagging anomalies, missing values, and schema changes before they corrupt downstream models. When prescription volumes from a specific data vendor drop suddenly, alerts trigger investigation rather than letting models train on incomplete data.
ML Model Development and Deployment
Most organizations separate model development from production deployment. Data scientists work in experimentation environments—Jupyter notebooks, MLflow tracking, feature engineering pipelines—testing dozens of model variants against historical data.
Promising models move into staging environments for validation against holdout datasets and compliance review. Only after passing both technical and regulatory validation do models deploy to production.
Production deployment increasingly uses real-time inference APIs. When a sales rep opens their tablet to review a physician’s profile, an API call hits the lead scoring model and returns a current score, next-best-action recommendation, and supporting rationale within milliseconds.
Model monitoring runs continuously in production, tracking prediction accuracy, data drift, and potential bias. When model performance degrades—say, a lead scoring model’s precision drops from 75% to 68%—alerts trigger retraining or investigation.
Popular ML Frameworks and Tools
Python dominates for model development, with scikit-learn handling traditional ML algorithms, TensorFlow or PyTorch for deep learning, and specialized libraries like XGBoost for gradient-boosted trees.
Natural language processing pipelines typically use transformer models—BERT variants for text classification, GPT-style models for content generation—often fine-tuned on pharmaceutical and medical literature to improve domain accuracy.
Graph neural networks handle physician network analysis, identifying influence patterns and peer effects in prescribing behavior. These models treat physicians as nodes and relationships—referral patterns, co-authorships, shared patients—as edges, then learn how prescribing behavior propagates through the network.
Measuring ML Impact: KPIs and Success Metrics
How do pharmaceutical companies know whether their machine learning investments deliver value? The answer requires careful measurement frameworks that connect ML outputs to business outcomes.
Model Performance Metrics
At the algorithm level, standard ML metrics apply: precision, recall, F1 scores for classification models; mean absolute error for regression models; area under the ROC curve for ranking models.
A lead scoring model with 70% precision means that when it flags a physician as high-priority, that physician converts 70% of the time—far better than the baseline conversion rate of 2-3%. That lift in precision directly translates to sales productivity gains.
But model performance metrics aren’t enough. A perfectly accurate model that takes three days to generate predictions has limited practical value.
Operational Efficiency Metrics
Machine learning should make marketing operations faster and cheaper. Key metrics include time saved in data integration, reduction in manual analysis hours, acceleration in campaign deployment, and decrease in wasted outreach to low-probability targets.
When ML-powered data mapping reduces integration time by 70%, that translates directly to analyst productivity and time-to-market for new campaigns.
Business Outcome Metrics
Ultimately, ML must drive revenue. The metrics that matter most to executives: increase in prescription volume, improvement in new patient starts, acceleration in market share growth, expansion in prescriber base, and overall marketing ROI.
The challenge is attribution. When multiple marketing channels touch a physician before they prescribe—email, sales rep visit, website interaction, speaker program—which channel deserves credit? Machine learning actually helps here too, using multi-touch attribution models to estimate each channel’s incremental contribution.
Common Pitfalls and How to Avoid Them
Implementing machine learning in pharma marketing involves predictable failure modes. Here are the most common and how to sidestep them.
Insufficient Data Quality
Machine learning models are only as good as their training data. When prescription datasets have 20% missing values, when physician identifiers don’t match across systems, when engagement tracking has gaps, models learn noise instead of signal.
The fix starts before any modeling: invest in data quality infrastructure, automated validation pipelines, and governance processes that maintain clean data over time. Boring work, but essential.
Overfitting to Historical Patterns
A model trained on 2018-2022 data might learn patterns that no longer hold in 2026. Physician preferences shift, competitive landscapes change, payer policies evolve. A model optimized for historical accuracy can fail spectacularly on current data.
The antidote is continuous retraining on recent data, monitoring for distribution drift, and incorporating external signals that flag when market conditions change substantially.
Ignoring Regulatory Constraints
Data scientists without pharma experience sometimes build systems that technically work but violate regulatory requirements. A content recommendation engine that suggests off-label studies. A lead scoring model that incorporates protected health information. An A/B test that lacks proper promotional review.
Prevention requires embedded compliance expertise in ML teams, regulatory review gates in deployment pipelines, and continuous training on pharmaceutical marketing standards.
Expecting Immediate ROI
Machine learning infrastructure requires upfront investment—data integration, model development, system integration, team training—with benefits that accrue over quarters and years rather than weeks.
Organizations that expect immediate returns often abandon implementations prematurely. The realistic timeline: 6-12 months for initial deployment, 12-24 months for measurable business impact, 24+ months for transformative value.
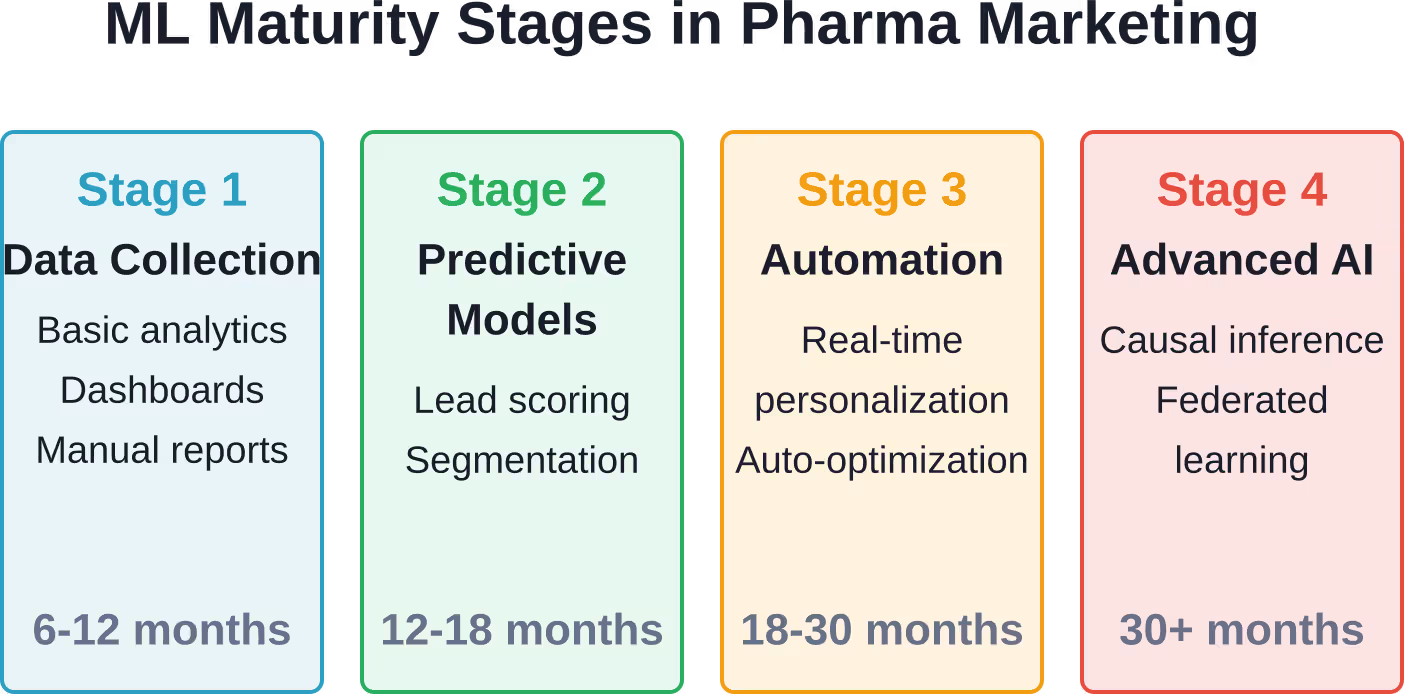
Emerging Trends Shaping the Next Wave
Machine learning in pharma marketing continues evolving rapidly. Several emerging trends will define the next 2-3 years.
Causal Machine Learning
Traditional ML predicts correlations: physicians with characteristic X tend to prescribe drug Y. But correlation doesn’t imply causation. Just because two patterns occur together doesn’t mean one causes the other.
Causal machine learning goes further, estimating cause-and-effect relationships from observational data. Instead of “physicians who attend webinars prescribe more,” causal models answer “would this physician prescribe more if we invited them to a webinar?”
Recent research demonstrates how causal machine learning can enhance drug development by identifying treatment effects from real-world data. The same techniques apply to marketing: understanding which interventions actually change prescribing behavior versus which simply correlate with it.
Federated Learning for Privacy-Preserving Analytics
Pharmaceutical companies often want to analyze data they can’t centralize due to privacy regulations. Patient-level data held by health systems. Physician behavioral data owned by different vendors. Competitive intelligence held by industry consortia.
Federated learning trains machine learning models on decentralized data without moving the data itself. The algorithm travels to where the data lives, trains locally, and returns only model updates—not raw data—to a central aggregation point.
This architecture enables collaborations previously impossible: multiple pharma companies pooling insights about physician preferences without sharing actual physician lists, or hospital systems contributing to patient outcome models without exposing protected health information.
Explainable AI and Interpretability
Early ML implementations often operated as black boxes: the model recommends action X, but nobody can explain why. That lack of transparency creates problems in regulated industries where decisions must be defensible.
The field of explainable AI develops techniques to make ML models interpretable. SHAP values quantify each feature’s contribution to a prediction. Attention mechanisms highlight which input data drove an output. Counterfactual explanations show what would need to change to alter a prediction.
For pharma marketing, this means sales reps can understand why the system recommends a specific physician visit, compliance teams can audit algorithmic decisions, and marketing leaders can build intuition about what drives model performance.
Generative AI for Content Creation
Large language models like GPT-4 and beyond are transforming content generation. These systems can draft medical education materials, generate personalized email copy, create FAQ responses, and summarize clinical studies—all at machine speed.
The pharmaceutical industry approaches generative AI cautiously given regulatory constraints. Content must be accurate, balanced, appropriately referenced, and compliant with promotional standards. Current implementations use generative AI for first drafts that human medical writers review and edit rather than for fully automated content publication.
But the productivity gains are substantial. If a medical writer can review and polish AI-generated drafts 3-4x faster than writing from scratch, content production capacity multiplies without proportional headcount growth.
Building Internal ML Capabilities vs. Vendor Solutions
Pharmaceutical companies face a build-versus-buy decision with machine learning implementations. Should they develop proprietary ML capabilities in-house or purchase packaged solutions from vendors?
The answer depends on strategic positioning and resource availability.
The Case for Building In-House
Proprietary ML capabilities become competitive differentiators when they incorporate unique data assets, encode specialized domain knowledge, or optimize for company-specific workflows that vendors can’t replicate.
A pharmaceutical company with exclusive access to longitudinal patient outcome data might build custom models that outperform vendor solutions trained on generic datasets. A company with unique sales force structures might develop targeting algorithms optimized for their specific go-to-market approach.
Building in-house also provides maximum flexibility and control—no vendor lock-in, no licensing fees scaling with usage, no delays waiting for vendor feature development.
The downside? Substantial upfront and ongoing investment. A production-grade ML team requires data engineers, ML engineers, data scientists, ML ops specialists, and domain experts—easily 15-25 FTEs for a comprehensive implementation.
The Case for Vendor Solutions
Packaged ML platforms offer faster time-to-value, lower upfront investment, and access to capabilities refined across multiple client implementations.
Vendors like Veeva, IQVIA, and specialized analytics firms provide pre-built models for physician targeting, engagement optimization, and campaign analytics—solutions that can deploy in months rather than years.
The tradeoff is reduced customization and ongoing licensing costs. Vendor models train on pooled data across multiple clients, which means broader datasets but less company-specific optimization. Feature development follows vendor roadmaps rather than internal priorities.
Many organizations adopt hybrid approaches: vendor solutions for commodity ML capabilities like basic lead scoring, in-house development for proprietary algorithms that drive competitive advantage.
Privacy, Ethics, and Responsible AI
Machine learning in pharmaceutical marketing raises important ethical questions around privacy, consent, algorithmic bias, and appropriate use of predictive technologies.
Physician Privacy and Consent
When ML models analyze physician prescribing patterns, engagement behaviors, and professional networks, whose data is it? Do physicians have a right to know they’re being profiled? Should they be able to opt out?
Current industry practice treats aggregated prescribing data as business intelligence rather than personal information requiring consent. But as profiling becomes more granular and predictive, the line blurs.
Some physicians find predictive targeting helpful—receiving information about treatments relevant to their patient population at appropriate times. Others perceive it as surveillance and manipulation.
The ethical path forward likely involves greater transparency: clearly communicating to physicians how their data gets used, what predictions get made, and providing meaningful control over data collection and profiling intensity.
Algorithmic Bias and Fairness
Machine learning models can perpetuate or amplify existing biases in training data. If historical prescription patterns reflect systemic inequities in healthcare access, models trained on that data might recommend reduced outreach to physicians serving underserved populations—deepening disparities.
Detecting and mitigating bias requires deliberate effort: analyzing model predictions across demographic segments, testing for disparate impact, and implementing fairness constraints that prevent models from discriminating based on protected characteristics.
The FDA’s guidance on AI in medical products emphasizes bias monitoring, and those principles extend logically to marketing applications. Responsible implementations audit for bias regularly and adjust models when problematic patterns emerge.
Transparency and Explainability
When an algorithm decides which physicians receive educational outreach about a new treatment option, that decision has real-world consequences for patient care. The system should be explainable—physicians and regulators should be able to understand why specific targeting decisions were made.
This requirement drives adoption of explainable AI techniques discussed earlier and argues against pure black-box models even when they might achieve marginally better accuracy.
Practical Next Steps for Organizations
For pharmaceutical marketing organizations considering or expanding machine learning implementations, here’s a pragmatic roadmap.
Assess Current Data Maturity
Successful ML requires foundational data capabilities. Before investing in algorithms, audit existing data infrastructure: What data sources do you currently integrate? How clean and complete is prescription data? What behavioral data gets captured? How well do identifiers link across systems?
If data infrastructure is immature—siloed datasets, poor quality, manual integration—invest there first. ML amplifies data quality; it doesn’t fix poor data.
Start with Narrow, High-Value Use Cases
Don’t try to revolutionize the entire marketing organization simultaneously. Identify 1-2 high-value, well-scoped use cases: physician lead scoring for a key product launch, email send-time optimization for a specific campaign, content recommendation for a medical affairs portal.
Prove value on focused applications, learn from implementation challenges, then expand to adjacent use cases once the initial projects demonstrate ROI.
Build Cross-Functional Teams
Effective ML implementations require collaboration across data science, marketing operations, IT, compliance, and commercial leadership. None of these functions succeeds in isolation.
Data scientists understand algorithms but need marketing experts to define business problems worth solving. Marketing teams understand physician engagement but need data scientists to build predictive models. Compliance teams understand regulatory constraints but need technical experts to implement guardrails.
Structure projects with explicit cross-functional ownership from the start.
Invest in Change Management
Machine learning often threatens existing workflows and roles. Sales reps accustomed to autonomy may resist algorithmic targeting recommendations. Marketing managers comfortable with creative intuition may distrust data-driven optimization.
Successful implementations invest heavily in change management: training teams to use ML tools effectively, clearly communicating how technology augments rather than replaces human judgment, and demonstrating tangible value that wins skeptics over.
Establish Governance and Monitoring
Before deploying ML to production, establish governance frameworks: Who reviews model recommendations before they reach field teams? What metrics trigger model retraining? How do compliance teams audit algorithmic decisions? What’s the escalation path when models behave unexpectedly?
These governance mechanisms prevent small issues from becoming major incidents.
FAQs
What types of machine learning models work best for pharmaceutical marketing?
The optimal model type depends on the specific use case. Gradient-boosted trees (XGBoost, LightGBM) excel at physician targeting and lead scoring because they handle mixed data types well and provide good interpretability. Neural networks work well for content recommendation and natural language processing tasks. Graph neural networks suit network analysis and peer influence modeling. For most tabular prediction problems in pharma marketing, ensemble methods combining multiple model types often outperform any single approach.
How much data is needed to train effective ML models for pharma marketing?
Minimum viable datasets typically require thousands of physicians with longitudinal prescription and engagement data spanning at least 12-24 months. For lead scoring models, having 500-1000 positive examples (physicians who converted) and similar numbers of negative examples usually suffices for initial models. More data always helps, but diminishing returns set in—a model trained on 50,000 physicians rarely performs drastically better than one trained on 10,000 if data quality is equivalent.
What’s the typical ROI timeline for machine learning in pharma marketing?
Most implementations require 6-12 months for initial deployment including data integration, model development, and system integration. Measurable business impact—improved targeting accuracy, higher engagement rates—typically appears within 12-18 months. Substantial ROI that clearly justifies the investment usually requires 18-24 months as models mature, teams adapt workflows, and compound effects accumulate. Organizations that abandon implementations before 18 months often do so prematurely, before the technology has time to prove value.
How do pharmaceutical companies handle off-label concerns with ML content recommendations?
Multiple safeguards prevent off-label promotion issues. First, ML models training on medical literature use filtered datasets that exclude off-label studies. Second, content libraries undergird recommendations only include pre-approved, on-label materials. Third, separate ML classifiers specifically trained to detect potential off-label content screen all recommendations before delivery. Fourth, human compliance review validates high-risk recommendations. These layered defenses make ML-driven content systems less prone to off-label violations than human-curated approaches.
Can small and mid-sized pharmaceutical companies benefit from ML, or is it only practical for large organizations?
Machine learning provides value at various scales, though implementations differ. Large pharma companies build comprehensive in-house platforms handling dozens of brands. Mid-sized companies typically adopt vendor solutions or focus ML efforts on 1-2 strategic products where competitive advantage matters most. Even smaller companies benefit from ML capabilities embedded in marketing automation platforms and CRM systems they already use—lead scoring, send-time optimization, basic personalization. The key is matching ML ambition to organizational resources and data assets rather than trying to replicate large pharma implementations at a smaller scale.
How does machine learning integrate with existing CRM and marketing automation systems?
Integration typically happens through APIs and data synchronization. ML models generate predictions—lead scores, next-best-actions, content recommendations—that get written back to CRM systems as custom fields. Marketing automation platforms then use those fields for segmentation, triggering, and personalization. Modern CRM platforms like Veeva CRM and Salesforce Health Cloud provide native integration points for ML model outputs. The technical integration is usually straightforward; the harder challenge is workflow design—determining how sales teams should act on ML recommendations and ensuring user interfaces surface insights effectively.
What regulatory guidance should companies follow when implementing ML in pharma marketing?
While the FDA has issued guidance on AI for drug development and medical devices, specific guidance for marketing applications remains limited. Companies typically follow broader pharmaceutical marketing regulations—FDA promotional guidance, PhRMA Code, HIPAA privacy rules—and apply them to ML implementations. Key principles include ensuring promotional materials (even if ML-generated or ML-selected) undergo appropriate review, maintaining audit trails for algorithmic decisions, protecting patient privacy in any patient-level analyses, and monitoring for bias or unintended consequences. Many companies establish internal AI governance committees that review ML applications before deployment to ensure regulatory alignment.
Conclusion
Machine learning represents the most significant operational transformation in pharmaceutical marketing since the introduction of prescription data analytics. The technology moves the discipline from intuition-driven mass marketing toward precision engagement optimized at the individual physician level.
But successful implementations require more than just algorithms and data. They demand careful attention to data quality, regulatory compliance, ethical considerations, organizational change management, and continuous monitoring. The companies winning with ML treat it as a long-term capability investment rather than a short-term technology project.
The competitive dynamics are clear: pharmaceutical organizations that master machine learning in marketing gain substantial advantages in market access speed, sales force productivity, and overall commercial effectiveness. Those that don’t risk falling behind competitors who leverage data more effectively.
The path forward isn’t about deploying every possible ML capability simultaneously. It’s about starting with focused, high-value applications, proving ROI, learning from early implementations, and gradually expanding machine learning’s role across marketing operations.
For organizations just beginning this journey, the time to start is now. Data accumulation takes time, model training requires iteration, and competitive advantages compound. The companies that will lead pharmaceutical marketing in 2030 are making foundational ML investments today.
Ready to explore how machine learning can transform your pharmaceutical marketing operations? Begin with a comprehensive assessment of your current data assets, identify 1-2 high-priority use cases, assemble cross-functional teams, and commit to the multi-year journey required for transformative impact. The technology is ready; the question is whether your organization is prepared to embrace it.