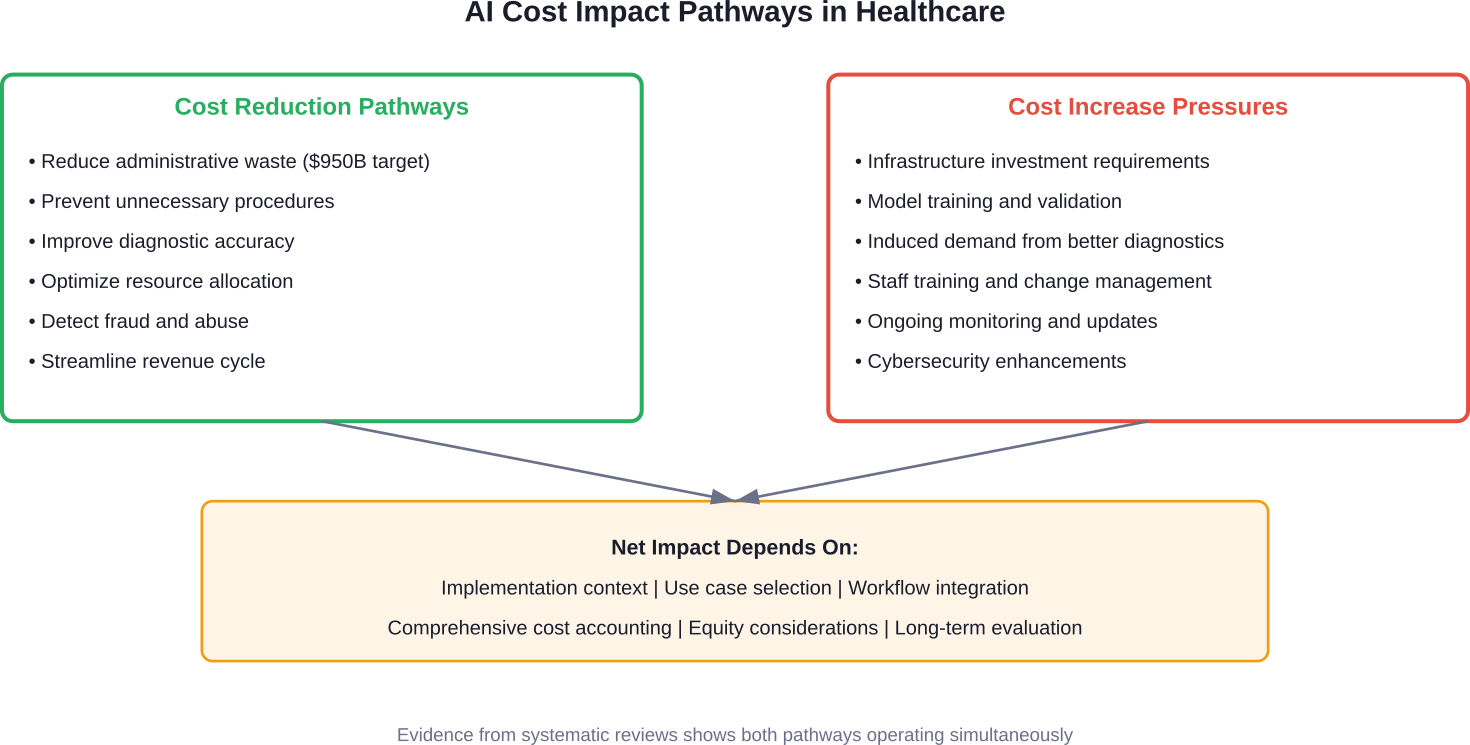
Quick Summary: Artificial intelligence is reshaping healthcare cost structures in complex ways. While AI shows promise in reducing administrative waste (estimated at $950 billion annually in 2019), improving diagnostic accuracy, and optimizing resource allocation, evidence from systematic reviews reveals a fragmented picture. Some AI interventions achieve cost-effectiveness ratios below accepted thresholds, yet many economic evaluations underreport infrastructure investments, indirect costs, and equity considerations—potentially overstating benefits.
Healthcare costs in the United States continue their relentless climb. And everyone’s looking for a solution.
Artificial intelligence has emerged as both a potential savior and another expensive technology demanding investment. The narrative swings wildly—AI will slash wasteful spending, or AI will drive costs even higher through induced demand and infrastructure requirements.
So what’s actually happening? The answer isn’t simple, but it’s critical for health systems, policymakers, and patients alike.
The Current State of Healthcare Spending and AI Adoption
Healthcare now sets the pace for enterprise AI adoption. That’s a remarkable shift for a sector long dismissed as a digital laggard. Fewer than one in 10 companies across the broader economy have implemented AI solutions, and most rely on general tools like enterprise ChatGPT rather than purpose-built systems.
Healthcare is different. Major health systems are deploying dozens of AI applications simultaneously. Advocate Health, for instance, evaluated over 225 AI solutions to select 40 use cases for deployment, including the largest implementation of Microsoft Dragon Copilot, along with imaging tools like Aidoc and Rad AI.
But here’s the thing—adoption doesn’t equal cost reduction. Not automatically.
Administrative and operational activities like workforce staffing, care coordination, billing and claims processing, and customer service contribute massively to U.S. healthcare costs. One estimate pegged these at $950 billion in 2019. That’s not clinical care. That’s the machinery running around clinical care.
AI targets this operational bloat aggressively. Yet the clinical side presents a more complicated picture.
How AI Actually Impacts Healthcare Costs: The Evidence
A systematic review published in 2025 examined cost-effectiveness, utility, and budget impact of clinical AI interventions across diverse healthcare settings. Nineteen studies spanning oncology, cardiology, ophthalmology, and infectious diseases provided the foundation.
The findings? AI improves diagnostic accuracy, enhances quality-adjusted life years, and reduces costs—largely by minimizing unnecessary procedures and optimizing resource use. Several interventions achieved incremental cost-effectiveness ratios well below accepted thresholds.
That sounds promising. But wait.
Many evaluations relied on static models that may overestimate benefits by not capturing the adaptive learning of AI systems over time. Additionally, indirect costs, infrastructure investments, and equity considerations were often underreported. The conclusion? Reported economic benefits may be overstated.
Another systematic review of economic evaluation studies reinforced this complexity. The integration of AI into healthcare systems has emerged as a transformative approach to addressing rising costs and inefficiencies, yet the evidence remains fragmented due to methodological heterogeneity.
Where AI Shows Real Cost Reduction Potential
Real talk: some applications demonstrate clear financial advantages.
Diagnostic imaging represents one of the strongest use cases. AI algorithms reduce false positives, prevent unnecessary biopsies and procedures, and accelerate throughput in radiology departments. The cost savings compound—fewer unnecessary follow-ups, reduced patient anxiety, optimized radiologist time.
Revenue cycle management shows similarly strong results. Generative AI models trained on specific tasks like medical coding demonstrate superior accuracy compared to general-purpose foundation models, while consuming far less computational resources. A study from the University of Michigan examined Clinical-BigBird models for heart failure and chronic kidney disease prediction, alongside GPT-4 prompts for ICD-labeling accuracy. The purpose-built models delivered better performance at dramatically lower operating costs.
Fraud, waste, and abuse detection presents another high-value target. The Centers for Medicare & Medicaid Services launched the Wasteful and Inappropriate Service Reduction (WISeR) Model in 2025 specifically to leverage AI and machine learning alongside human clinical review. The goal? Ensure timely and appropriate Medicare payment for select items and services while protecting taxpayers from unnecessary procedures.
According to CMS, combining the speed of technology with experienced clinicians helps bring Medicare into the 21st century by testing a streamlined prior authorization process.
Where AI Might Actually Increase Costs
Now, this is where it gets interesting.
One health economist interviewed in March 2026 raised a critical concern: AI may drive health costs up, not down. The mechanism? Induced demand.
When diagnostic tools become more accurate and accessible, they get used more frequently. More diagnoses lead to more treatments. Some of those treatments deliver genuine value. Others represent marginal interventions with questionable cost-effectiveness.
There’s historical precedent. Healthcare delivery reform initiatives like accountable care organizations and primary care medical homes generated significant optimism. Unfortunately, the savings from these programs in many cases proved small or even zero—maybe 1% or 2% from the more successful programs.
AI faces similar dynamics. Improved diagnostic capability doesn’t automatically translate to system-wide cost reduction if it primarily expands the volume of services delivered rather than substituting efficient processes for wasteful ones.
Infrastructure costs represent another substantial factor. Implementing AI requires data systems integration, model training and validation, ongoing monitoring and updates, staff training, and cybersecurity enhancements. Many economic evaluations underreport or completely omit these components.
Government Initiatives Targeting AI-Driven Cost Control
The federal government isn’t sitting on the sidelines. CMS has launched multiple initiatives to harness AI for cost containment while maintaining or improving care quality.
The WISeR Model: AI Meets Prior Authorization
The Wasteful and Inappropriate Service Reduction (WISeR) Model represents CMS’s most ambitious AI-focused cost control initiative to date. Announced in June 2025, this voluntary model encourages care navigation toward safe and evidence-supported best practices.
The approach combines enhanced technologies—specifically AI and machine learning—with human clinical review. The goal isn’t to replace clinical judgment but to flag potentially unnecessary or inappropriate services before Medicare pays for them.
Sound familiar? It’s essentially AI-enhanced prior authorization.
Critics worry this could create new administrative burdens and delays in care. Proponents argue that protecting beneficiaries from unnecessary procedures while safeguarding taxpayer dollars justifies the additional scrutiny.
The model’s effectiveness will depend heavily on implementation details not yet fully specified.
Broader Health Technology Modernization
CMS’s Health Technology Ecosystem initiative takes a wider view. The agency describes America’s healthcare system as plagued by complexity, high costs, and fragmentation—placing strain on patients, providers, and the national budget. Outdated infrastructure and disconnected data make the problem worse.
The strategy focuses on empowering Medicare beneficiaries through greater access to innovative health technologies. AI sits at the center of this modernization effort, but success requires addressing fundamental interoperability and data standardization challenges.
Making health tech great again—as CMS frames it—demands more than deploying algorithms. It requires redesigning workflows, incentive structures, and data ecosystems.
Clinical AI Cost-Effectiveness: What the Research Actually Shows
Let’s dig into specific findings from economic evaluations.
Oncology Applications
Cancer diagnosis and treatment planning represent high-stakes, high-cost areas where AI demonstrates measurable impact. Studies examining AI-assisted pathology, imaging interpretation, and treatment selection show improved diagnostic accuracy translating to fewer unnecessary biopsies and more targeted therapy selection.
The economic benefit derives primarily from avoiding ineffective treatments and their associated toxicities, rather than reducing the cost of effective treatments. Quality-adjusted life years improve while unnecessary healthcare utilization decreases—a genuine win-win scenario.
But implementation costs matter. Pathology departments require digital infrastructure, pathologists need training, and validation processes demand time and expertise. Studies that omit these factors overstate net benefits.
Cardiology and Chronic Disease Management
Predictive models for heart failure, chronic kidney disease, and other chronic conditions aim to identify high-risk patients before acute events occur. The economic logic is compelling: prevent a hospitalization, save tens of thousands of dollars.
The University of Michigan study mentioned earlier developed Clinical-BigBird models specifically for heart failure and chronic kidney disease prediction. These models outperformed general-purpose large language models on accuracy metrics while consuming far less computational resources.
Lower computational costs translate directly to lower operational expenses. A purpose-built model might cost pennies per prediction, while a GPT-4 API call costs substantially more and delivers inferior results for specialized clinical tasks.
That said, predictive models only generate value when predictions trigger effective interventions. Identifying high-risk patients means nothing if care coordination systems can’t deliver appropriate preventive care.
Ophthalmology and Screening Programs
Diabetic retinopathy screening with AI-enabled automated grading systems demonstrates one of the clearest cost-benefit profiles. The technology allows non-specialist settings to conduct screenings, expanding access while reducing reliance on scarce ophthalmologist time.
Economic evaluations consistently show favorable incremental cost-effectiveness ratios. The intervention prevents blindness—a devastating outcome with enormous quality-of-life and economic consequences—through early detection and treatment.
Importantly, ophthalmology AI often operates in well-defined, high-volume screening contexts with clear outcome metrics. This contrasts with more complex clinical scenarios where AI’s value proposition becomes murkier.
| Clinical Area | Primary AI Application | Cost Impact Mechanism | Evidence Quality |
|---|---|---|---|
| Oncology | Imaging interpretation, pathology | Avoid unnecessary procedures, target therapy | Moderate (infrastructure costs often unreported) |
| Cardiology | Predictive risk modeling | Prevent acute events, optimize resource use | Moderate (depends on intervention effectiveness) |
| Ophthalmology | Diabetic retinopathy screening | Expand access, prevent costly complications | Strong (well-defined screening context) |
| Radiology | Image analysis, workflow optimization | Reduce false positives, improve throughput | Strong (workflow benefits well-documented) |
| Revenue Cycle | Medical coding, claims processing | Reduce administrative labor, improve accuracy | Moderate to Strong (direct cost metrics available) |
The Operational AI Opportunity: Lessons From Other Industries
Healthcare has lagged other sectors in adopting operational AI technologies. Financial services, manufacturing, and retail deployed AI for workforce optimization, supply chain management, and customer service years before healthcare began similar efforts.
Why the delay? Healthcare’s unique characteristics create barriers: fragmented data systems, regulatory complexity, risk aversion, and fee-for-service incentives that don’t reward operational efficiency.
But those barriers are cracking. Health systems now recognize that operational AI—distinct from clinical AI—offers substantial cost reduction potential without the clinical risk considerations that slow adoption of diagnostic and treatment algorithms.
Workforce Staffing and Scheduling
Airlines mastered dynamic workforce optimization decades ago. Retailers use sophisticated algorithms to match staffing levels to predicted demand.
Healthcare is finally catching up. AI-driven staffing tools predict patient volumes, acuity levels, and resource requirements with increasing accuracy. The financial impact? Reduced overtime costs, lower contract labor spending, and better matching of skills to patient needs.
One large health system implementing AI staffing optimization reported labor cost savings of several percentage points—modest sounding, but representing millions of dollars annually at scale.
Supply Chain and Inventory Management
Hospital supply chain inefficiencies cost the industry billions annually. Expired supplies, emergency orders at premium prices, stockouts of critical items—all entirely preventable with better systems.
AI applications imported from manufacturing and retail optimize inventory levels, predict demand fluctuations, and identify opportunities for standardization and bulk purchasing. The savings don’t require clinical validation or FDA approval. They just require implementation discipline.
Customer Service and Administrative Functions
Conversational AI handles appointment scheduling, insurance verification, prescription refills, and basic patient inquiries. The technology isn’t perfect, but it’s increasingly capable of managing routine interactions that previously required human staff time.
The cost equation here is straightforward: AI operational costs versus human labor costs. For high-volume, low-complexity tasks, AI wins decisively. The challenge lies in maintaining service quality and ensuring smooth handoffs to humans for complex situations.
The Infrastructure Cost Reality: What Economic Models Miss
Here’s what systematic reviews consistently find: economic evaluations underreport infrastructure costs, indirect expenses, and long-term maintenance requirements.
Why does this happen? Several reasons.
First, many studies focus narrowly on direct intervention costs—the cost of running the algorithm, essentially. They compare AI diagnostic costs to human diagnostic costs without accounting for the entire technology stack required to deploy AI at scale.
Second, researchers often conduct evaluations using pilot or research settings where infrastructure already exists for other purposes. The marginal cost of adding one more AI application to an existing research computing environment vastly understates the cost a typical community hospital would face implementing the same technology.
Third, vendor partnerships and research grants often subsidize pilot implementations. Published economic evaluations may reflect subsidized costs rather than sustainable operational costs.
What Infrastructure Actually Costs
Implementing clinical or operational AI requires:
- Electronic health record integration and API development
- Data warehousing and preprocessing pipelines
- Model training infrastructure (often cloud-based compute)
- Inference serving infrastructure
- Monitoring and alerting systems
- Security and compliance controls
- Staff training and ongoing education
- Workflow redesign and change management
For a large health system, these components can easily require seven-figure investments before the first AI algorithm delivers clinical or operational value.
That doesn’t mean AI lacks economic viability. It means accurate cost-benefit analysis must account for total cost of ownership over multi-year periods, not just algorithmic operating costs.
The Build vs Buy Decision
Health systems face a critical choice: build custom AI solutions in-house or purchase vendor products.
Building in-house offers customization and control but requires substantial technical talent—data scientists, machine learning engineers, software developers, DevOps specialists. Top-tier talent commands premium compensation, and healthcare systems compete with technology companies for the same people.
Buying vendor solutions shifts infrastructure burden to the vendor but introduces subscription costs, vendor lock-in risks, and less customization. Vendor pricing models vary wildly, from per-user subscriptions to per-transaction fees to percentage-of-savings arrangements.
Neither approach is universally superior. The optimal choice depends on organizational technical capability, use case specificity, and scale of deployment.

Keep Healthcare AI Costs Grounded From the Start
Healthcare AI projects tend to get expensive when scope, data requirements, and validation processes grow without clear limits. AI Superior works across the full development cycle, including data preparation, model building, fine-tuning, and deployment, with attention to how systems will actually be used in practice. Instead of pushing for larger models or extended training by default, the focus is on building solutions that meet clinical or operational needs without unnecessary complexity. This helps reduce repeated testing cycles, avoid overuse of compute, and keep systems manageable over time.
In healthcare, cost is closely tied to how well the system fits its purpose. When models are aligned with real workflows and constraints, both development and long-term operation become easier to control. If you want to keep AI spend predictable in a healthcare setting, contact AI Superior and review how your project is scoped before it expands.
Equity Considerations in AI Healthcare Economics
Cost-effectiveness analysis typically examines average effects across populations. But AI interventions may deliver uneven benefits—and costs—across demographic groups.
Several equity concerns deserve attention.
Algorithmic Bias and Differential Performance
AI models trained primarily on data from one demographic group may perform poorly for others. A diagnostic algorithm optimized on data from academic medical centers serving affluent populations might miss pathology patterns common in underserved communities.
The economic consequences extend beyond fairness concerns. Differential performance means cost-effectiveness varies by population. An intervention may be highly cost-effective for the majority population while being cost-ineffective or even harmful for minorities.
Comprehensive economic evaluation should include subgroup analyses examining performance and cost-effectiveness across race, ethnicity, socioeconomic status, and geography. Many published studies omit these analyses entirely.
Access and Digital Divide Issues
AI-enabled virtual care, remote monitoring, and digital-first service delivery promise cost savings. But they require patients to have internet access, digital literacy, and appropriate devices.
Populations lacking these resources face exclusion from AI-enabled care pathways, potentially exacerbating existing disparities. The cost savings achieved through digital transformation may come partly at the expense of underserved populations who get relegated to more expensive traditional care pathways—or forego care altogether.
Workforce Impacts
AI automation affects healthcare workers differently based on their roles, educational credentials, and labor market positions.
Radiologists face direct competition from AI diagnostic tools. Medical coders see their work increasingly automated. Administrative staff in billing and scheduling face similar pressures.
Meanwhile, AI creates demand for new roles: clinical informaticists, AI trainers and validators, and algorithm oversight specialists. These positions typically require advanced education and technical skills, potentially accessible only to already-privileged workers.
The net employment effect remains uncertain, but the distributional impact clearly varies. Cost savings from AI-driven workforce optimization may concentrate economic harm among specific worker groups while benefits accrue broadly to health systems and patients.
Real-World Implementation Challenges
Economic models assume rational implementation. Reality is messier.
Workflow Integration Friction
An AI algorithm might deliver technically impressive performance in isolation while creating workflow chaos when deployed in actual clinical settings.
If an AI alert system generates too many false positives, clinicians develop alert fatigue and ignore warnings—including the occasional true positive. If an AI recommendation requires clinicians to switch between multiple systems, the time cost may exceed any efficiency gain.
Effective AI implementation requires human-centered design, extensive user testing, and iterative refinement. These activities cost money and time, rarely captured in economic evaluations.
Data Quality and Interoperability
AI is only as good as its input data. Healthcare data is notoriously messy: missing values, inconsistent coding, unstructured text, siloed systems that don’t communicate.
Cleaning and harmonizing data for AI applications represents a major hidden cost. Organizations spend countless hours on data pipelines, standardization efforts, and quality improvement before AI models can even be trained.
Interoperability initiatives aim to address these challenges, but progress remains slow. Each health system operates different EHR configurations, creating a fragmented landscape that resists standardization.
Regulatory and Reimbursement Uncertainty
FDA regulation of clinical AI continues evolving. The pathway for algorithm approval, ongoing monitoring requirements, and post-market surveillance obligations all affect implementation costs.
Reimbursement represents another moving target. When do payers cover AI-enhanced diagnostics? Do they pay separately for AI interpretation, or must it be bundled into existing payment codes? How do value-based payment models account for AI-driven cost savings?
These uncertainties create risk that conservative organizations may find prohibitive.
| Implementation Challenge | Cost Impact | Mitigation Strategy |
|---|---|---|
| Workflow integration friction | Lost productivity, user resistance | Human-centered design, iterative testing |
| Data quality issues | Pipeline development, cleaning labor | Invest in data governance infrastructure |
| Interoperability gaps | Custom integration work | Adopt standards, participate in HIEs |
| Regulatory uncertainty | Compliance overhead, approval delays | Engage early with FDA, monitor guidance |
| Reimbursement ambiguity | Revenue risk, ROI uncertainty | Document outcomes, engage payers early |
| Vendor lock-in | Switching costs, negotiating leverage | Prioritize open standards, data portability |
What Health System Leaders Need to Know
For executives evaluating AI investments, several principles emerge from the evidence.
Start With High-Value, Lower-Risk Use Cases
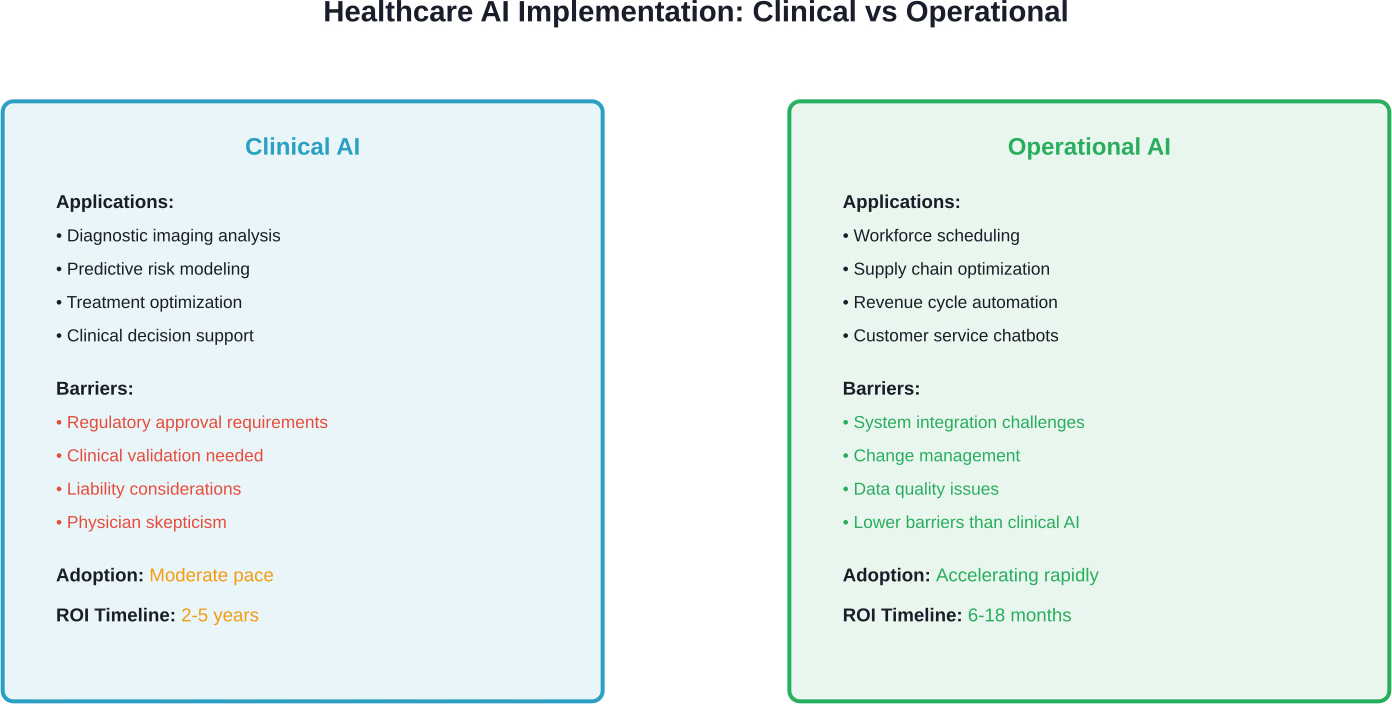
Operational AI applications—workforce scheduling, supply chain optimization, revenue cycle automation—offer clearer ROI with fewer clinical risk considerations than diagnostic or treatment algorithms.
These use cases deliver measurable cost savings on shorter timelines, building organizational confidence and capability for more complex clinical AI deployments.
Demand Comprehensive Cost Accounting
Vendor pitches emphasize algorithmic performance and potential savings. Insist on total cost of ownership analysis including infrastructure, integration, training, maintenance, and opportunity costs.
Be skeptical of ROI projections based on pilot studies or best-case scenarios. Ask what percentage of claimed savings were actually realized by existing customers, and request references from organizations with similar characteristics to yours.
Invest in Data Infrastructure First
AI is fundamentally dependent on data quality and availability. Organizations lacking solid data governance, integration capabilities, and analytics infrastructure should address those foundational elements before deploying complex AI applications.
The infrastructure investment may seem unglamorous compared to cutting-edge AI algorithms, but it determines whether AI initiatives succeed or fail.
Redesign Workflows, Don’t Just Add Technology
Effective AI implementation requires workflow redesign, not just technology insertion into existing processes. The greatest value comes from fundamentally rethinking how work gets done, with AI enabling new approaches rather than simply automating old ones.
This requires engaging frontline staff, investing in change management, and accepting that optimization takes time and iteration.
Measure What Matters
Establish clear metrics before implementation: specific cost categories targeted for reduction, quality measures that must be maintained or improved, equity indicators, and user satisfaction benchmarks.
Track these metrics rigorously. Many AI projects claim success based on technical performance metrics while failing to deliver meaningful business or clinical value.
The Policy and Reimbursement Landscape
Government policy shapes AI’s economic viability in healthcare through regulation, reimbursement, and direct initiatives.
CMS Innovation Center Models
The WISeR Model represents just one of many Innovation Center efforts. CMS continuously tests new payment and service delivery models, increasingly incorporating AI and digital health technologies.
Participating in these models offers health systems opportunities to pilot AI applications with some financial protection, data support, and regulatory clarity. The models also influence broader reimbursement policy as successful innovations scale.
Commercial Payer Approaches
Commercial health plans pursue AI in parallel tracks: using AI internally for claims processing, utilization management, and fraud detection, while also evaluating coverage policies for AI-enhanced clinical services.
Coverage policy remains inconsistent. Some plans cover AI-enhanced diagnostics under existing codes. Others require specific medical necessity documentation. A few experimental contracts tie reimbursement to AI-driven quality or cost metrics.
This fragmentation creates challenges for providers trying to implement AI consistently across diverse payer contracts.
International Perspectives
Healthcare systems outside the U.S. face different economic constraints and incentives. National health services in the U.K. and elsewhere conduct systematic health technology assessments for AI interventions, weighing cost-effectiveness from a societal perspective.
These evaluations often apply stricter cost-effectiveness thresholds than U.S. commercial decisions, potentially limiting AI adoption where evidence remains preliminary. But they also provide more consistent, evidence-based frameworks for evaluating economic value.
Looking Forward: What the Next Five Years May Bring
Healthcare AI is still in its early innings. Several trends will shape cost impacts through 2030 and beyond.
Foundation Models and Generative AI
Large language models and multimodal foundation models promise broader capabilities with less custom training for each task. This could dramatically reduce the cost of deploying AI for new use cases.
However, foundation models also introduce new challenges: higher computational costs for inference, intellectual property and data privacy concerns, and the risk of confident-sounding but inaccurate outputs.
The University of Michigan research comparing Clinical-BigBird to GPT-4 suggests purpose-built models may retain advantages for specific healthcare tasks, at least in cost efficiency if not always in capability.
Regulatory Evolution
FDA continues developing frameworks for AI/ML-based medical devices, including approaches for continuously learning algorithms. Clearer regulatory pathways should reduce compliance uncertainty, potentially lowering the risk premium organizations assign to AI investments.
Conversely, stricter post-market surveillance requirements could increase ongoing compliance costs.
Value-Based Care Alignment
As healthcare payment shifts from fee-for-service toward value-based models, AI’s ability to improve outcomes while reducing costs becomes more directly aligned with financial incentives.
Organizations bearing financial risk for population health have stronger motivation to invest in AI tools for care coordination, predictive intervention, and resource optimization.
This alignment could accelerate adoption and drive focus toward high-value use cases.
Equity Requirements
Expect growing policy emphasis on equity considerations in AI deployment. CMS and other payers may require evidence of equitable performance across populations as a condition of coverage or participation in payment models.
This could increase evaluation costs but also ensure that economic benefits don’t come at the expense of vulnerable populations.
Frequently Asked Questions
Does AI actually reduce healthcare costs or increase them?
The answer is context-dependent. AI demonstrates clear cost reduction potential in operational areas like revenue cycle management, workforce scheduling, and supply chain optimization, with some health systems reporting labor cost savings of several percentage points. Clinical AI shows promise in preventing unnecessary procedures and improving diagnostic accuracy, which can reduce costs. However, AI also creates cost pressures through infrastructure investments, induced demand from better diagnostics, and ongoing maintenance requirements. Systematic reviews find that many economic evaluations underreport these indirect costs, potentially overstating net benefits. The overall impact depends on implementation quality, use case selection, and comprehensive cost accounting.
What are the main cost components of implementing AI in healthcare?
Beyond the direct cost of AI algorithms, organizations face substantial expenses for EHR integration and API development, data warehousing and preprocessing, model training infrastructure (often cloud-based), inference serving systems, monitoring and alerting platforms, security and compliance controls, staff training, and workflow redesign. For large health systems, these infrastructure components can require seven-figure investments before realizing value. Vendor solutions shift some infrastructure burden but introduce subscription costs and potential lock-in. Both build and buy approaches require significant change management investment to ensure effective adoption.
How does the WISeR Model use AI to control Medicare costs?
The Wasteful and Inappropriate Service Reduction (WISeR) Model, launched by CMS in June 2025, combines AI and machine learning with human clinical review to identify potentially unnecessary or inappropriate services before Medicare pays for them. The voluntary model targets wasteful care by leveraging technology speed alongside experienced clinicians to streamline prior authorization processes. According to CMS, the approach helps protect beneficiaries from unnecessary procedures while safeguarding taxpayer dollars. The model’s effectiveness will depend on balancing fraud prevention against administrative burden and care access concerns.
Why do some AI economic evaluations overstate cost savings?
Systematic reviews identify several methodological issues. Many evaluations rely on static models that don’t capture adaptive learning of AI systems over time, potentially overestimating long-term benefits. Studies often focus narrowly on direct intervention costs while underreporting infrastructure investments, indirect expenses, and maintenance requirements. Pilot implementations frequently occur in research settings with subsidized infrastructure or vendor partnerships that don’t reflect sustainable operational costs. Additionally, evaluations often omit equity considerations and subgroup analyses, missing differential performance across populations. Comprehensive total cost of ownership analysis over multi-year periods provides more accurate assessment than algorithmic operating costs alone.
Where has AI shown the clearest cost-effectiveness in healthcare?
Diabetic retinopathy screening demonstrates one of the strongest cost-benefit profiles, with AI-enabled automated grading allowing non-specialist settings to conduct screenings while preventing blindness and its enormous economic consequences. Revenue cycle management shows similarly clear benefits, with purpose-built models for medical coding delivering superior accuracy at dramatically lower computational costs than general-purpose foundation models. Operational applications in workforce scheduling and supply chain optimization deliver measurable savings on shorter timelines without clinical risk considerations. Radiology workflow optimization reduces false positives and improves throughput with well-documented benefits. These use cases share characteristics of well-defined tasks, high volumes, and clear outcome metrics.
How do equity considerations affect AI healthcare economics?
AI models may perform differently across demographic groups, meaning cost-effectiveness varies by population. An intervention might be highly cost-effective for majority populations while cost-ineffective or harmful for minorities if trained primarily on non-representative data. AI-enabled virtual care and remote monitoring require internet access, digital literacy, and devices—excluding populations lacking these resources and potentially exacerbating disparities. Workforce impacts also vary, with automation affecting medical coders and administrative staff while creating demand for technical roles accessible mainly to already-privileged workers. Comprehensive economic evaluation should include subgroup analyses across race, ethnicity, socioeconomic status, and geography, though many published studies omit these entirely.
What should health system leaders prioritize when implementing AI?
Start with operational AI applications offering clearer ROI and fewer clinical risks—workforce scheduling, supply chain optimization, revenue cycle automation—to build organizational confidence and capability. Demand comprehensive total cost of ownership analysis including infrastructure, integration, training, and maintenance costs, not just vendor-claimed savings. Invest in data governance, integration capabilities, and analytics infrastructure as prerequisites for successful AI deployment. Redesign workflows around AI rather than inserting technology into existing processes, engaging frontline staff throughout. Establish clear metrics before implementation covering cost targets, quality maintenance, equity indicators, and user satisfaction. Track rigorously to ensure AI delivers meaningful business and clinical value beyond technical performance.
Conclusion: Navigating the AI Cost Paradox
Artificial intelligence in healthcare presents a genuine paradox. The technology offers legitimate pathways to cost reduction through operational efficiency, diagnostic accuracy, and resource optimization. Simultaneously, it introduces new cost pressures from infrastructure investment, induced demand, and implementation complexity.
Neither the optimistic vision of AI slashing healthcare spending nor the pessimistic view of AI as just another expensive technology driving costs higher captures the full reality.
The actual economic impact depends on execution. Organizations that invest in data infrastructure, prioritize high-value use cases, redesign workflows thoughtfully, and account comprehensively for total costs can realize meaningful savings and quality improvements. Those that chase technological novelty without strategic discipline will likely see disappointing returns.
Government initiatives like the WISeR Model and broader CMS modernization efforts signal policy alignment toward AI-enabled cost control, but implementation details matter enormously. Balancing fraud prevention against administrative burden and care access remains challenging.
The evidence base continues maturing. Systematic reviews reveal both AI’s clinical promise and the economic complexity often underappreciated in early evaluations. Dynamic modeling, equity analysis, and comprehensive cost accounting will produce more reliable guidance for decision-makers.
For now, healthcare leaders should approach AI with informed optimism: enthusiastic about genuine opportunities, realistic about challenges, and disciplined about measurement. The technology won’t solve healthcare’s cost crisis alone, but it represents a powerful tool when applied strategically.
The organizations that navigate this complexity successfully—building capability, selecting wisely, implementing thoughtfully, and measuring rigorously—will gain competitive advantages in an increasingly value-driven healthcare landscape.
Ready to evaluate AI opportunities for your organization? Start with comprehensive needs assessment, honest capability inventory, and total cost of ownership analysis. The investment in strategic planning will pay dividends in implementation success.