Quick Summary: Machine learning is revolutionizing Alzheimer’s disease diagnosis by analyzing neuroimaging data, genetic markers, and clinical assessments with unprecedented accuracy. Recent studies show AI models achieving 96.19% accuracy on MRI-based detection and 99.82% on hybrid multimodal approaches, enabling earlier intervention than traditional methods. These technologies identify subtle biomarker changes years before symptoms appear, offering hope for better patient outcomes.
Alzheimer’s disease represents one of the most devastating neurodegenerative conditions affecting millions worldwide.
Traditional diagnostic methods often catch the disease too late. By the time clinical symptoms become obvious, irreversible brain damage has already occurred.
Machine learning changes this equation entirely.
These computational approaches analyze patterns in brain imaging, genetic data, and clinical assessments that human clinicians simply can’t detect. The results speak for themselves: recent models achieve accuracy rates exceeding 96%, identifying at-risk individuals years before traditional methods would catch the disease.
But here’s the thing—not all machine learning approaches work equally well. The type of data, the algorithm choice, and the training methodology all dramatically impact diagnostic accuracy.
Understanding Alzheimer’s Disease and the Diagnostic Challenge
Alzheimer’s disease accounts for more than 60% of patients in dementia outpatient clinics, making it the most prevalent neurodegenerative cause of dementia. The disease doesn’t strike randomly—it follows predictable age-related patterns.
Early diagnosis matters tremendously. Once clinical symptoms appear, neuronal damage has typically progressed beyond repair. Traditional diagnostic workflows rely on cognitive tests, clinical assessments, and imaging—but these methods lack the sensitivity to catch subtle early changes.
Machine learning models excel precisely where traditional methods fail: detecting minute patterns across massive datasets.
The Five Stages of Alzheimer’s Progression
Alzheimer’s disease doesn’t appear overnight. It progresses through distinct stages:
| Stage | Characteristics | Diagnostic Challenge |
|---|---|---|
| Preclinical Alzheimer’s | No symptoms, biomarker changes only | Undetectable by clinical assessment alone |
| Mild Cognitive Impairment (MCI) | Noticeable memory issues, daily function intact | Difficult to distinguish from normal aging |
| Mild Dementia | Memory loss affects daily activities | Often diagnosed at this stage traditionally |
| Moderate Dementia | Significant cognitive decline, assistance needed | Clear diagnosis, treatment limited |
| Severe Dementia | Loss of communication, full-time care required | Advanced damage, intervention ineffective |
Machine learning models target the first two stages—preclinical and MCI—where intervention can still make a difference.
How Machine Learning Models Diagnose Alzheimer’s Disease
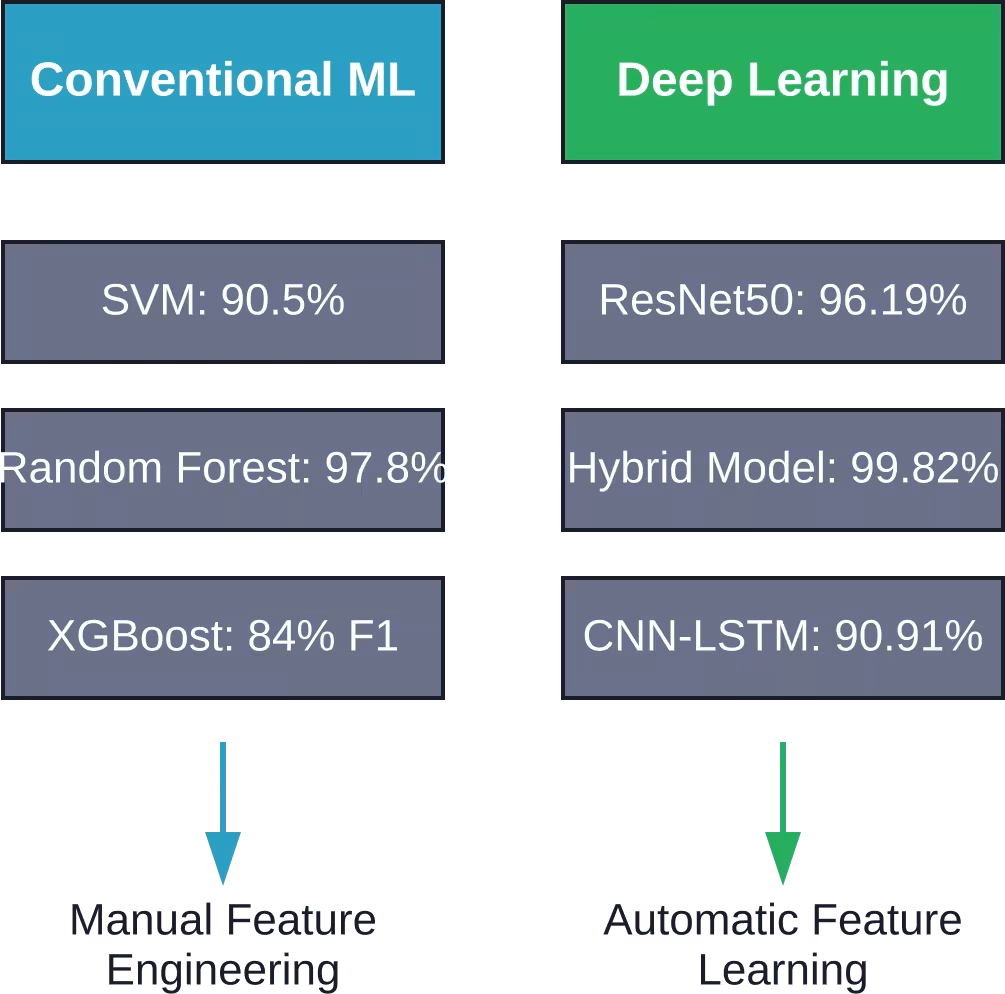
Machine learning approaches fall into two broad categories: conventional algorithms and deep learning networks. Each offers distinct advantages depending on the data type and diagnostic goal.
The core process remains consistent: train the model on labeled data (patients with known diagnoses), then test its ability to correctly classify new cases.
Conventional Machine Learning Approaches
Support Vector Machines (SVM) have shown remarkable performance in Alzheimer’s classification. These algorithms find the optimal boundary separating different diagnostic categories in high-dimensional feature space.
Recent research demonstrates SVM models achieving competitive performance for multiclass classification (with reported F1 scores of 90.7% for multiclass classification) across different disease stages.
Random Forest models take a different approach. They combine multiple decision trees, each trained on slightly different data subsets. This ensemble method reduces overfitting and improves generalization.
Random Forest models have demonstrated strong performance on Alzheimer’s classification tasks, with one study achieving 84.4% accuracy when cognitive data was included.
Other conventional approaches include:
- Logistic Regression for binary classification tasks
- XGBoost for gradient-boosted decision trees
- k-Nearest Neighbors for similarity-based classification
- Naive Bayes for probabilistic predictions
Deep Learning Networks
Deep learning models process raw data—like brain scans—without manual feature engineering. Convolutional Neural Networks (CNNs) excel at image analysis, making them ideal for MRI and PET scan interpretation.
ResNet50 and MobileNetV2 architectures have achieved 96.19% accuracy when analyzing MRI scans from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) dataset.
Here’s where it gets interesting: hybrid models combining multiple deep learning architectures can push accuracy even higher. One hybrid approach reached 99.82% accuracy on the National Alzheimer’s Coordinating Centre (NACC) dataset.
CNN-LSTM models combine spatial pattern recognition with temporal sequence analysis. This architecture achieved 90.91% accuracy using non-invasive near-infrared spectroscopy, offering a portable diagnostic option.
Neuroimaging Data: MRI and PET Scans
Brain imaging provides the richest data source for machine learning models. MRI scans reveal structural changes—shrinking hippocampus, cortical thinning, and white matter alterations. PET scans show metabolic activity and protein deposits like amyloid plaques and tau tangles.
Machine learning models extract features from these scans that correlate with disease progression.
MRI-Based Classification
Structural MRI captures anatomical changes in brain regions affected by Alzheimer’s. The hippocampus shrinks early in the disease process, making volumetric measurements particularly valuable.
But measuring hippocampal volume manually takes time and introduces variability. Machine learning automates this process and identifies additional subtle patterns across the entire brain.
Recent models using ResNet50 and MobileNetV2 architectures achieved 96.19% accuracy distinguishing between normal cognition, mild cognitive impairment, and Alzheimer’s disease on the ADNI dataset.
The process works like this:
- Preprocessing standardizes brain scans (alignment, skull removal, intensity normalization)
- The CNN extracts spatial features across different brain regions
- Classification layers map these features to diagnostic categories
- The model outputs probability scores for each diagnosis
PET Imaging and Tau Pathology
PET scans detect molecular changes before structural damage appears. Amyloid-beta plaques and tau tangles—the hallmark proteins of Alzheimer’s—show up clearly on PET imaging.
The FDA approval of Tauvid, a PET tracer targeting tau pathology, opened new diagnostic possibilities. Tau accumulation correlates more closely with cognitive decline than amyloid deposits alone.
Machine learning models trained on PET data can predict disease progression years in advance. Combined PET-MRI approaches leverage both molecular and structural information for maximum accuracy.
Multimodal Neuroimaging Approaches
The strongest results come from combining multiple imaging modalities. MRI shows where the brain has shrunk. PET shows where toxic proteins have accumulated. Together, they paint a complete picture.
Multimodal models achieved 95.52% accuracy identifying AD stages and progression from MCI using combined MRI and clinical data.
Real talk: single-modality models work well for binary classification (AD versus normal). But for staging the disease and predicting progression, multimodal approaches dominate.
Genetic Data and Risk Prediction
Genetic variants influence Alzheimer’s risk long before symptoms appear. The APOE-ε4 allele represents the strongest genetic risk factor, but dozens of other loci contribute.
Machine learning models can detect subtle genetic patterns that traditional genome-wide association studies miss.
Beyond APOE: Novel Genetic Loci
Traditional statistical approaches identified major risk genes like APOE. Machine learning goes further, uncovering complex interactions between multiple genetic variants.
Gradient Boosting Machines (GBMs) applied to genome-wide data from 41,686 individuals successfully replicated all known genome-wide significant variants and identified 6 novel loci. These include variants mapping to ARHGAP25, LY6H, COG7, SOD1, and ZNF597.
The GBM model achieved an area under the curve (AUC) of 0.692 for distinguishing cases from controls—comparable to traditional polygenic risk scores (PRS) which scored 0.689.
But here’s what matters: machine learning models captured 22% of associations from larger meta-analyses that wouldn’t have reached statistical significance in the training set alone.
Combining Genetic and Imaging Data
Genetic data detects risk before symptoms. Imaging data shows actual brain changes. Combining both improves prediction accuracy dramatically.
MRI reflects anatomical changes already underway. Genetic data identifies risk years or decades before the first structural changes appear. Models trained on both data types can stratify patients into risk categories and predict progression timelines.
This multimodal genetic-imaging approach enables truly personalized risk assessment.
Clinical and Biomarker Data Integration
Cognitive assessments and biomarker measurements provide crucial diagnostic information. The Clinical Dementia Rating (CDR) scale, Mini-Mental State Examination (MMSE), and other neuropsychological tests quantify cognitive function.
Cerebrospinal fluid biomarkers—amyloid-beta 42, total tau, and phosphorylated tau—correlate strongly with pathology.
The Critical Role of Cognitive Assessments
One recent study evaluated four machine learning models for AD stage classification with and without cognitive assessment data. The results were striking.
Random Forest achieved 84.4% accuracy when cognitive data was included. Without it, performance dropped significantly across all models.
SHAP analysis revealed that models primarily rely on functional scores like the Clinical Dementia Rating—Sum of Boxes when available. Remove those scores, and the models correctly shift to biological markers: PET imaging of amyloid burden (FBB, AV45) and hippocampal atrophy measurements.
This demonstrates something important: machine learning models learn medically sensible patterns. They don’t just memorize data—they discover the same relationships clinicians recognize.
Predicting Disease Progression
Diagnosing current disease state matters. But predicting future progression matters more.
Can machine learning predict which MCI patients will progress to Alzheimer’s dementia within four years? Recent research shows it can.
SVM models achieved F1 scores of 88% for binary progression prediction and 72.8% for multiclass progression categories over a 4-year period.
This capability transforms clinical decision-making. Doctors can identify high-risk patients who need aggressive monitoring and early intervention trials.
Model Explainability and Clinical Trust
Accuracy alone doesn’t guarantee clinical adoption. Doctors need to understand why a model makes specific predictions.
Black-box algorithms that spit out diagnoses without explanation create trust problems. If a model can’t explain its reasoning, clinicians won’t rely on it for patient care.
SHAP and LIME for Model Interpretation
SHapley Additive exPlanations (SHAP) quantify how much each feature contributes to individual predictions. This approach reveals which brain regions, genetic variants, or cognitive scores drove a particular diagnosis.
LIME (Local Interpretable Model-agnostic Explanations) takes a different approach. It approximates the complex model’s behavior locally around a specific prediction using a simpler, interpretable model.
Studies using SHAP analysis on SVM models identified memory function, judgment, communication ability, and orientation as the most important factors determining AD risk. These align perfectly with clinical knowledge—the model learned medically sensible patterns.
Rule Extraction Approaches
Some researchers extract explicit rules from trained models. These human-readable if-then statements help clinicians understand decision boundaries.
Two rule-extraction methods—class rule mining and stable and interpretable rule sets—generated understandable rules from complex classifiers. Domain experts validated these rules, confirming they captured genuine medical relationships rather than spurious correlations.
This validation process matters tremendously. It demonstrates that high-performing models aren’t just memorizing training data—they’re discovering real diagnostic patterns.

Discuss Your Alzheimer’s ML Project With AI Superior
For teams working on machine learning in Alzheimer’s diagnosis, AI Superior can help turn an early idea into a structured AI project. Their work covers AI consulting, machine learning, data science, AI software development, proof of concept development, and model evaluation, which fits projects where clinical data, model quality, and practical implementation need careful planning.
AI Superior can support teams with:
- Defining the ML use case and project scope
- Reviewing available datasets and data requirements
- Building a proof of concept or prototype
- Developing machine learning and data science models
- Testing model performance and reliability
- Planning integration into existing software or internal workflows
- Supporting AI product development from early concept to deployment
For Alzheimer’s diagnosis projects, this may be relevant for teams working with clinical records, imaging-related data, cognitive assessment data, biomarkers, or other structured medical datasets.
Contact AI Superior to discuss the project.
Key Datasets Driving Alzheimer’s ML Research
Machine learning models need large, well-labeled datasets. Several major repositories enable Alzheimer’s research.
ADNI: Alzheimer’s Disease Neuroimaging Initiative
ADNI represents the gold standard for neuroimaging research. It combines longitudinal MRI and PET scans with cognitive assessments, genetic data, and biomarker measurements from thousands of participants.
The dataset tracks participants over years, enabling progression prediction studies. Most published accuracy benchmarks reference ADNI data, making results comparable across studies.
NACC: National Alzheimer’s Coordinating Center
NACC aggregates data from Alzheimer’s Disease Research Centers across the United States. With 169,408 records and 1024 features, it dwarfs most other datasets.
The hybrid AI model achieved 99.82% accuracy trained on NACC data—though that exceptional performance required careful feature selection and model tuning.
Other Important Repositories
Kaggle hosts various Alzheimer’s datasets for research and competition purposes.
MIRIAD (Minimal Interval Resonance Imaging in Alzheimer’s Disease) provides multiple time-point MRI scans suitable for longitudinal studies.
Each dataset has strengths and limitations. ADNI offers the most comprehensive multimodal data. NACC provides the largest sample size. Kaggle datasets vary in quality but enable rapid prototyping.
Clinical Implementation Challenges
Research accuracy and real-world performance differ significantly. Models achieving 95%+ accuracy on carefully curated research datasets often stumble when applied to routine clinical data.
The Research-to-Practice Gap
Research datasets undergo extensive quality control. Scans follow standardized protocols. Missing data gets carefully imputed or excluded.
Clinical routine data is messier. Scanning protocols vary between hospitals. Image quality fluctuates. Missing values appear frequently.
One study specifically evaluated MRI-based machine learning performance on real clinical data versus research datasets. The accuracy drop was substantial—models trained on pristine research data struggled with real-world variability.
Regulatory and Validation Requirements
FDA approval requires demonstrating safety and efficacy on diverse patient populations. Models trained primarily on research volunteers may not generalize to broader demographics.
Validation on external datasets—completely separate from training data—provides the truest performance measure. Many published studies only report internal cross-validation results, which overestimate real-world accuracy.
Integration with Clinical Workflows
Even accurate models fail if they disrupt clinical workflows. Radiologists won’t use tools that require hours of preprocessing or manual image annotation.
Successful clinical implementation demands:
- Automated preprocessing pipelines that handle variable image quality
- Fast inference times compatible with clinical scheduling
- Clear, actionable output reports
- Integration with existing PACS and EMR systems
- Explainable predictions that support clinical decision-making
Emerging Trends and Future Directions
The field continues advancing rapidly. Several promising directions could further improve diagnostic accuracy and clinical utility.
Foundation Models and Transfer Learning
Large-scale pretraining on diverse medical imaging data creates foundation models. These can be fine-tuned for Alzheimer’s diagnosis with smaller disease-specific datasets.
This approach addresses the perpetual challenge of limited labeled data. Instead of training from scratch, models start with knowledge learned from millions of brain scans across various conditions.
Federated Learning for Privacy-Preserving Collaboration
Patient privacy regulations limit data sharing between institutions. Federated learning enables model training across multiple sites without centralizing sensitive data.
Each hospital trains a local model on its own data. Only model updates—not patient data—get shared centrally. This approach could unlock datasets currently siloed by privacy constraints.
Liquid Biomarkers and Accessible Diagnostics
The CNN-LSTM model achieving 90.91% accuracy using near-infrared spectroscopy points toward a future of portable, non-invasive diagnostics.
Blood-based biomarker tests combined with machine learning could enable screening in primary care settings. This accessibility would dramatically expand early detection beyond specialized memory clinics.
Longitudinal Modeling and Trajectory Prediction
Current models mostly perform cross-sectional classification. Future approaches will better model disease trajectories—predicting not just current state but the shape of future decline.
Recurrent neural networks and temporal convolution models can capture progression dynamics. These could identify fast versus slow progressors, enabling personalized treatment planning.
Practical Considerations for Healthcare Systems
Hospitals and healthcare systems considering machine learning implementation face several practical questions.
Cost-Benefit Analysis
MRI and PET scanning carry significant costs. Machine learning doesn’t eliminate imaging—it extracts more value from existing scans.
The economic case depends on whether earlier detection actually improves outcomes. If disease-modifying treatments become available, early diagnosis becomes economically justified. Until then, the value lies primarily in better clinical trial recruitment and patient planning.
Expertise Requirements
Implementing machine learning systems requires collaboration between radiologists, neurologists, data scientists, and IT specialists.
Most hospitals lack in-house machine learning expertise. Third-party solutions and cloud-based diagnostic platforms could fill this gap—but they introduce data privacy and vendor lock-in concerns.
Ethical Considerations
Predictive models raise difficult questions. Should patients be told they’ll likely develop Alzheimer’s when no effective treatment exists?
Genetic risk predictions compound these concerns. High-risk individuals may face insurance discrimination or psychological distress from knowing their likely future.
Clear guidelines around disclosure, counseling, and patient autonomy need to accompany technological advancement.
Comparing ML Performance Across Studies
Published accuracy figures vary dramatically. Understanding why helps interpret research claims.
| Study Approach | Accuracy | Dataset | Task Complexity |
|---|---|---|---|
| SVM multiclass classification | 90.5% | Various | Multiple disease stages |
| Random Forest with cognitive data | 97.8% | Research cohort | Full feature set |
| ResNet50 MRI analysis | 96.19% | ADNI | 3-class (CN/MCI/AD) |
| Hybrid multimodal model | 99.82% | NACC | Binary (CN/AD) |
| CNN-LSTM near-infrared | 90.91% | Portable device | Non-invasive screening |
| Progression prediction (4-year) | 88% F1 | Longitudinal | Binary progression |
Several factors explain these differences:
- Task difficulty: Binary classification (AD versus normal) is easier than multiclass staging or progression prediction.
- Dataset quality: Curated research datasets enable higher accuracy than heterogeneous clinical data.
- Feature availability: Models with full clinical, imaging, and genetic data outperform single-modality approaches.
- Class balance: Datasets with equal numbers of patients in each category yield higher accuracy than imbalanced real-world distributions.
The 95% classification accuracy threshold for distinguishing AD from MCI or CN represents a meaningful benchmark that multiple studies have achieved or exceeded.
Limitations of Current Approaches
Despite impressive accuracy figures, machine learning in Alzheimer’s diagnosis faces real constraints.
Dataset Limitations
Most research datasets under-represent minority populations, rural patients, and individuals with comorbidities. Models trained on these datasets may not generalize to diverse real-world populations.
Longitudinal datasets track participants for years but include relatively small sample sizes. This limits power for rare outcome prediction.
Biological Heterogeneity
Alzheimer’s disease isn’t a single condition. Different subtypes involve varying patterns of protein accumulation and neurodegeneration.
Current models mostly ignore this heterogeneity, treating all AD cases as equivalent. Subtype-specific models could improve accuracy and treatment matching.
Interpretability Challenges
Despite SHAP and LIME advances, deep learning models remain partially opaque. Clinicians want to know not just which features matter, but why specific patterns indicate disease.
Neuroscience understanding of why certain imaging patterns correlate with cognitive decline remains incomplete. Machine learning identifies these patterns but doesn’t explain underlying mechanisms.
Frequently Asked Questions
How accurate is machine learning for diagnosing Alzheimer’s disease?
Recent studies demonstrate accuracy rates between 90% and 99%, depending on the data types used and task complexity. MRI-based models using ResNet50 and MobileNetV2 architectures achieved 96.19% accuracy on the ADNI dataset, while hybrid multimodal models reached 99.82% on NACC data. Binary classification tasks (distinguishing Alzheimer’s from normal cognition) generally achieve higher accuracy than multiclass staging or progression prediction.
What types of data do machine learning models use for Alzheimer’s diagnosis?
Machine learning models integrate multiple data sources including structural MRI scans showing brain atrophy, PET imaging revealing amyloid and tau protein deposits, genetic variants like APOE-ε4, cognitive assessment scores from tests like CDR and MMSE, cerebrospinal fluid biomarkers, and demographic information. Multimodal approaches combining several data types consistently outperform single-source models.
Can machine learning predict Alzheimer’s before symptoms appear?
Yes, machine learning models can identify preclinical Alzheimer’s and predict progression from mild cognitive impairment to dementia. Genetic data detects risk years before structural brain changes appear, while sensitive imaging analysis reveals subtle biomarker changes before clinical symptoms emerge. Recent models achieved 88% F1 scores predicting which MCI patients would progress to Alzheimer’s dementia within four years.
Are machine learning diagnostic tools approved for clinical use?
Most machine learning models for Alzheimer’s diagnosis remain research tools rather than FDA-approved clinical devices. The research-to-practice gap remains substantial—models achieving high accuracy on curated research datasets often perform worse on routine clinical data. Regulatory approval requires demonstrating safety and efficacy across diverse patient populations with varying data quality.
What is the difference between conventional machine learning and deep learning for Alzheimer’s diagnosis?
Conventional machine learning algorithms like Support Vector Machines and Random Forest require manual feature engineering—experts must identify and extract relevant measurements from raw data. Deep learning models automatically learn features directly from raw images or genetic sequences. Deep learning typically achieves higher accuracy on complex image data, while conventional methods often perform well on structured clinical data and provide more interpretable results.
How do researchers make machine learning models explainable to doctors?
Explainability methods like SHAP (SHapley Additive exPlanations) and LIME quantify how much each feature contributes to individual predictions, revealing which brain regions, genetic variants, or cognitive scores influenced a diagnosis. Rule extraction techniques generate human-readable if-then statements from complex models. These approaches help clinicians understand and validate model reasoning, building trust necessary for clinical adoption.
What datasets are available for Alzheimer’s machine learning research?
The Alzheimer’s Disease Neuroimaging Initiative (ADNI) provides the most comprehensive multimodal dataset combining longitudinal MRI and PET scans with cognitive assessments, genetic data, and biomarkers. The National Alzheimer’s Coordinating Center (NACC) offers the largest sample size with 169,408 records. Kaggle hosts various datasets used in approximately 15% of research articles, while MIRIAD provides multiple time-point MRI scans for longitudinal studies.
Conclusion
Machine learning has fundamentally transformed Alzheimer’s disease diagnosis. Models now achieve accuracy rates exceeding 96%, identifying at-risk individuals years before traditional methods would detect the disease.
The strongest results come from multimodal approaches integrating neuroimaging, genetic data, cognitive assessments, and biomarkers. Deep learning architectures like ResNet50 automatically extract subtle patterns from brain scans, while conventional algorithms like Random Forest and SVM excel at structured clinical data.
But accuracy alone doesn’t guarantee clinical impact.
The research-to-practice gap, regulatory requirements, interpretability demands, and ethical considerations around predictive diagnosis all present real challenges. Models validated on pristine research datasets must prove themselves on messy clinical routine data before widespread adoption becomes feasible.
The future looks promising. Foundation models, federated learning, portable biomarker devices, and longitudinal trajectory modeling will further improve diagnostic capabilities. As disease-modifying treatments emerge, the value of early detection will become undeniable.
For healthcare systems considering implementation, the key questions aren’t technical—the algorithms work. The questions are practical: Does earlier diagnosis improve patient outcomes? Can existing workflows accommodate these tools? What expertise and infrastructure does implementation require?
The technology has arrived. Now comes the harder work of translating research breakthroughs into routine clinical practice that genuinely helps patients and families facing this devastating disease.
The algorithms can see what human clinicians miss. The question is whether healthcare systems will adapt to leverage that capability effectively.