Quick Summary: Machine learning is revolutionizing public health through enhanced disease surveillance, predictive outbreak modeling, resource allocation, and personalized interventions. The CDC’s AI initiatives have already demonstrated measurable impact, including $3.7 million in labor cost savings and a 527% ROI from GenAI deployment. ML applications span diagnosis, treatment optimization, antimicrobial resistance tracking, and health equity identification—transforming how agencies detect threats, respond to emergencies, and protect populations.
Public health agencies face an unprecedented challenge: mountains of data, limited staff, and threats that evolve faster than traditional methods can track them. Machine learning offers a way forward.
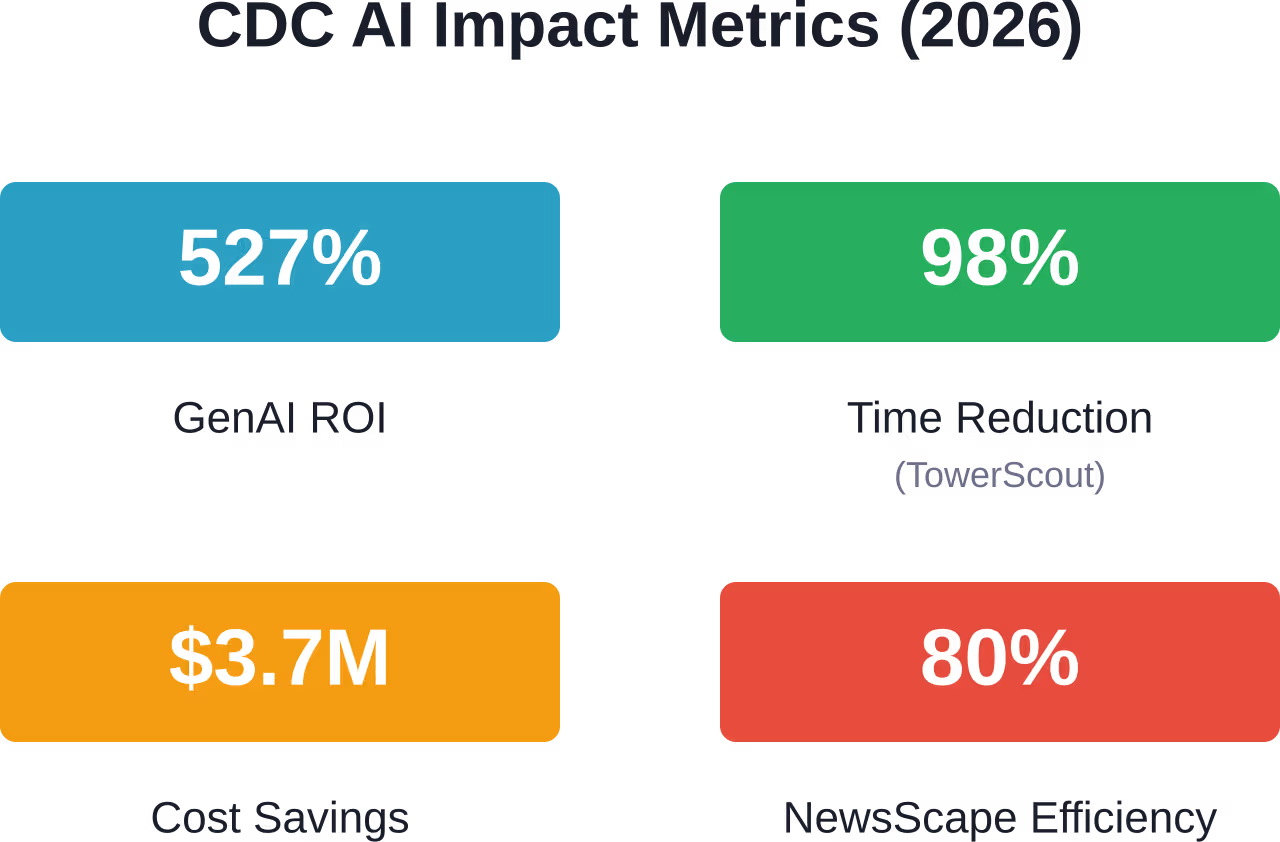
The transformation isn’t theoretical anymore. According to the CDC, their GenAI chatbot deployment has saved an estimated $3.7 million in labor costs with a 527% return on investment as of 2026. That’s real money, real efficiency gains, and real proof that ML can scale public health capacity.
But the story goes deeper than cost savings. ML algorithms are detecting disease outbreaks in real time, identifying at-risk populations before crises emerge, and personalizing interventions in ways that were impossible just five years ago.
This guide breaks down how machine learning is reshaping public health—what’s working, what the evidence shows, and where the field is headed.
What Machine Learning Brings to Public Health
Machine learning is a subset of artificial intelligence that learns patterns from data without explicit programming for every scenario. Feed an algorithm thousands of patient records, and it can start predicting who’s at highest risk for complications. Show it satellite imagery, and it can identify environmental health hazards.
Traditional statistical methods require researchers to specify relationships upfront. ML flips that model—it finds relationships in the data itself, even ones humans might miss.
The applications fall into several categories:
- Surveillance and outbreak detection: Real-time analysis of symptom data, social media signals, and clinical reports to catch emerging threats early
- Predictive modeling: Forecasting disease spread, hospital admissions, and resource needs before they happen
- Diagnostic support: Pattern recognition in medical imaging, lab results, and patient histories to improve accuracy
- Resource allocation: Optimization algorithms that determine where to deploy limited staff, vaccines, or testing capacity
- Health equity identification: Finding underserved populations and disparities hidden in complex datasets
Here’s the thing though—ML isn’t replacing epidemiologists or public health workers. It’s amplifying what they can accomplish with limited time and budgets.
CDC’s AI Transformation: Real Numbers, Real Impact
The Centers for Disease Control and Prevention became the first federal agency to deploy a generative AI chatbot to all staff. The results speak for themselves.
That single initiative contributed to over $3.7 million in estimated labor cost savings with a 527% return on investment. More than 30 federal agencies have since requested CDC’s GenAI guidance.
But CDC’s AI work extends far beyond chatbots:
TowerScout: Computer Vision for Legionella Prevention
TowerScout uses computer vision to analyze satellite imagery and automatically detect cooling towers that may harbor Legionella bacteria—the cause of Legionnaires’ disease.
The impact? A 98% reduction in identification time. What previously took four hours per area now takes five minutes. During an outbreak response, that speed difference can save lives.
National Syndromic Surveillance Program
This system uses machine learning algorithms to analyze real-time symptom data from emergency departments across the country. It detects outbreaks and monitors health trends as they emerge, not days or weeks later when case reports trickle in through traditional channels.
NewsScape: Automated Information Extraction
CDC’s NewsScape system uses natural language processing to scan global news sources for disease mentions, travel alerts, and health emergencies. It increased the efficiency of information extraction by 80 percent with respect to a baseline scenario, helping public health teams act on insights that might otherwise be overlooked.
These aren’t pilot projects or proof-of-concepts. They’re operational systems protecting public health right now.
Disease Surveillance and Outbreak Prediction
Traditional disease surveillance relies on case reports flowing from clinicians to local health departments to state agencies to the CDC. That process takes time—often days or weeks.
ML flips the timeline. Algorithms can detect unusual patterns in emergency department visits, prescription drug sales, social media posts, or search engine queries in near real-time.
One study using state surveillance data on substance use, sexually transmitted diseases, and community characteristics identified high-priority areas for HIV prevention programs through supervised learning models. Of the areas flagged by the algorithm, 79% did not have implemented programs—revealing significant gaps in coverage.
Outbreak forecasting has seen particularly strong results. LSTM and GRU neural network models consistently delivered accuracy rates up to 93% in forecasting dengue and influenza outbreaks, outperforming traditional methods like ARIMA or logistic regression.
What Makes ML Effective for Surveillance
Machine learning excels at surveillance for several reasons:
- Pattern recognition across noise: Public health data is messy. ML algorithms can detect meaningful signals amid incomplete records, reporting delays, and background variation.
- Multi-source integration: Traditional methods struggle to combine disparate data types. ML can fuse clinical data, environmental sensors, demographic information, and behavioral signals into unified risk assessments.
- Temporal modeling: Recurrent neural networks and similar architectures capture how disease patterns evolve over time, not just snapshots.
The National Syndromic Surveillance Program processes symptom data from thousands of emergency departments simultaneously. No human team could manually review that volume—but ML algorithms handle it continuously.
Diagnosis and Treatment Optimization
ML applications in clinical decision support have grown rapidly. Analysis of ML and AI publications in the public health domain found that diagnosis was a common application area, followed by treatment.
An optimized ensemble model combining deep learning with traditional ML achieved 92% prediction accuracy for diseases including acute hepatitis B, malaria, and meningitis based on laboratory test results.
For bloodstream infections—a major cause of hospital mortality—ML models achieved an AUROC of 0.82 in predicting poor outcomes, allowing clinicians to identify high-risk patients earlier.
Antimicrobial Resistance: A Critical Application
Antimicrobial resistance represents one of the most serious global health threats. Projections indicate that without effective intervention, AMR could lead to 10 million deaths annually by 2050 and cost the global economy up to $100 trillion.
Hospital-acquired resistant infections result in significant lost hospital bed days and substantial costs annually. Carbapenem resistance among K. pneumoniae isolates represents a significant public health challenge.
ML is proving valuable for:
- Predicting which patients will develop resistant infections based on prior antibiotic exposure, comorbidities, and local resistance patterns
- Optimizing antibiotic selection by matching patient characteristics to historical treatment outcomes
- Identifying transmission patterns within hospitals to target infection control measures
- Forecasting resistance trends to guide empiric treatment guidelines
Random forests achieved the best performance in 56% of disease prediction tasks across multiple studies, particularly for conditions with specific treatment options like diabetes.
Resource Allocation and Health Equity
Public health departments operate under severe resource constraints. Which neighborhoods need additional vaccine clinics? How many contact tracers should each jurisdiction receive? Where should limited testing capacity be deployed?
ML optimization algorithms can answer these questions based on disease burden, population density, access barriers, and predicted uptake—factors too complex for manual allocation.
Identifying Health Equity Gaps
Here’s where ML gets really interesting. Traditional analysis might show that certain ZIP codes have higher disease rates. ML can dig deeper—identifying specific combinations of poverty, environmental exposures, healthcare access, and social determinants that create concentrated risk.
Analysis of ML publications in public health found only 105 focused on health equity—the smallest category examined. That gap represents both a challenge and an opportunity.
When properly designed with equity considerations built in, ML can reveal disparities that aggregate statistics miss. Mental health prediction systems based on natural language processing and wearable data achieved up to 91% accuracy in detecting stress and depression—potentially identifying at-risk individuals before crisis points.
But there’s a catch. ML models trained on biased data will amplify those biases. If training data underrepresents certain populations, the model performs poorly for those groups. Health equity applications require deliberate attention to representative datasets and fairness metrics.
Implementation Science and Policy Evaluation
How do public health departments know which interventions actually work in real-world settings? Implementation science seeks those answers—and ML is expanding what’s possible.
Traditional evaluation methods compare outcomes before and after an intervention. ML approaches can predict what will work best, for whom, under what circumstances, and with what level of support needed.
Strategic Implementation Framework
ML techniques apply across implementation stages:
| Stage | ML Application | Example |
|---|---|---|
| Setting the stage | Context analysis and barrier identification | Predicting which clinics will face adoption challenges based on staffing, resources, and population characteristics |
| Active implementation | Real-time monitoring and adaptation | Identifying when program fidelity is drifting and what modifications maintain effectiveness |
| Monitor and sustain | Outcome prediction and sustainability assessment | Forecasting which sites will maintain programs long-term versus those needing additional support |
Support vector machines, random forests, and neural networks have all been applied to implementation questions. The key advantage: these models can handle the complexity of real-world implementation where dozens of factors interact.
Policy Evaluation at Scale
Evaluating public health policies traditionally requires extensive data collection, long follow-up periods, and careful control group selection. ML enables faster, more nuanced evaluation.
One study used multiple ML algorithms including support vector machines to evaluate smoking cessation interventions, analyzing which patient characteristics and program features predicted success. The models identified specific subgroups where standard approaches failed and alternative strategies worked better.
Decision trees proved particularly valuable for policy evaluation because they’re interpretable—policymakers can see exactly which factors drive outcomes and at what thresholds.

Use ML for Public Health Data Analysis With AI Superior
Public health systems rely on large-scale data from multiple sources, including demographics, healthcare records, and statistical reporting. Machine learning helps identify patterns and improve data interpretation. AI Superior provides AI consulting and machine learning development for data-driven healthcare applications.
Need a Machine Learning Solution for Public Health Data?
AI Superior can support projects involving:
- Custom machine learning model development for large datasets
- Statistical and predictive data analysis
- Integration of ML solutions into existing platforms
👉Get in touch with AI Superior to discuss your public health machine learning project.
Challenges and Limitations
ML in public health faces significant hurdles. Understanding them is just as important as understanding the applications.
Data Quality and Availability
ML models are only as good as their training data. Public health data comes with unique problems:
- Incompleteness: Not everyone accesses healthcare. Not all conditions get reported. Surveillance systems have gaps.
- Bias: If certain populations are underrepresented in health records, models trained on that data will perform poorly for those groups.
- Fragmentation: Data exists in dozens of disconnected systems—hospital records, insurance claims, vital statistics, disease registries, environmental monitoring. Integrating these sources is technically and legally complex.
Transparency and Trust
Many powerful ML models are “black boxes”—they produce accurate predictions but don’t explain why. Public health decisions affect people’s lives. “The algorithm says so” isn’t sufficient justification for closing a clinic or targeting an intervention.
Analysis of AI and ML publications found that while more than half used open-source software, only one-in-six (~16%) authors made their detailed algorithms publicly available. That lack of transparency hinders validation and trust-building.
Explainable AI methods are emerging but still lag behind predictive performance. The field needs models that are both accurate and interpretable.
Equity Risks
Real talk: ML can worsen health disparities if deployed carelessly. Models trained predominantly on data from well-resourced healthcare systems may fail when applied to underserved communities.
Algorithmic bias isn’t just a technical problem. It reflects and can amplify existing structural inequities in healthcare access, research participation, and data collection.
Addressing this requires:
- Diverse training datasets that represent all populations served
- Fairness metrics evaluated across demographic groups
- Community engagement in algorithm design and deployment decisions
- Regular audits for disparate impact
Workforce and Capacity
Public health departments need staff who understand both epidemiology and ML. That skillset is rare and expensive.
Smaller jurisdictions especially struggle. Building and maintaining ML systems requires data scientists, software engineers, and computational infrastructure. Not every health department has those resources.
Cloud-based platforms and shared services can help, but capacity building remains a major barrier to widespread adoption.
Ethical Considerations and Governance
WHO has emphasized the importance of establishing safety, effectiveness, and appropriate governance for AI systems in health. Their guidance identifies key principles:
- Protect human autonomy: ML systems should support—not replace—human judgment in public health decision-making.
- Promote human well-being and safety: Algorithms must be rigorously tested before deployment, with ongoing monitoring for unintended consequences.
- Ensure transparency and explainability: Those affected by ML-driven decisions deserve to understand how those decisions were made.
- Foster responsibility and accountability: Clear lines of accountability must exist when algorithms err or cause harm.
- Ensure inclusiveness and equity: ML applications should reduce—not widen—health disparities.
- Promote responsive and sustainable systems: ML tools should be designed for long-term maintenance and adaptation as populations and threats change.
Regulatory Landscape
WHO has released considerations for regulation of AI in health, emphasizing the need to establish safety and effectiveness while rapidly making appropriate systems available to those who need them.
The challenge: traditional regulatory frameworks weren’t designed for algorithms that learn and evolve. An ML model that performs well in trials might drift in real-world deployment as data distributions shift.
Continuous monitoring and recalibration are necessary—but how do regulatory agencies oversee that? The governance models are still being worked out.
The Future: Where ML and Public Health Are Headed
Several trends are accelerating:
Generative AI Integration
CDC’s success with GenAI chatbots is just the beginning. Large language models can summarize medical literature, draft public communications, and answer routine queries—freeing staff for complex work only humans can do.
But generative AI introduces new risks. These models can “hallucinate” false information convincingly. Safeguards are critical.
Federated Learning
This approach trains ML models across multiple institutions without sharing raw data—addressing privacy concerns while enabling large-scale learning. Hospitals and health departments can collaboratively build models while keeping patient data local.
Real-Time Genomic Surveillance
ML analysis of pathogen genomes is becoming fast enough for outbreak response. During future pandemics, algorithms will track variant emergence, predict immune escape, and guide vaccine updates in near real-time.
Wearables and Continuous Monitoring
Consumer devices generate continuous physiological data. ML algorithms can detect infection before symptoms appear, monitor chronic disease management, and identify mental health deterioration. The privacy and consent implications are enormous.
Climate and Environmental Health
ML models are being developed to predict how climate change will shift disease patterns—where mosquito-borne illnesses will spread, which communities face heat vulnerability, and how wildfires will affect respiratory health.
Practical Steps for Public Health Agencies
Organizations looking to implement ML should follow a structured approach:
Start with Data Infrastructure
Before building models, get data systems in order. That means:
- Standardized data formats across departments and systems
- Electronic data pipelines that reduce manual entry
- Data governance policies covering privacy, security, and sharing
- Quality assurance processes to catch errors before they corrupt models
Boring? Absolutely. Essential? Also yes.
Identify High-Value Use Cases
Not every problem needs ML. Focus on applications where:
- Prediction accuracy matters more than explanation (e.g., outbreak forecasting)
- Patterns are too complex for traditional methods
- Scale requires automation (e.g., screening thousands of reports)
- Real-time response provides clear value
CDC’s TowerScout is a perfect example—computer vision solved a specific, high-value problem (finding cooling towers) that was tedious and slow manually.
Build Multidisciplinary Teams
Effective ML in public health requires:
- Epidemiologists who understand disease dynamics and causal inference
- Data scientists who can build and tune models
- Software engineers who can deploy systems reliably
- Ethicists who can identify potential harms
- Community stakeholders who understand local context
No single person has all those skills. Teams do.
Validate Rigorously Before Deployment
Test models on held-out data. Check performance across demographic groups. Run pilot studies with human review. Iterate based on feedback.
Then monitor continuously after deployment because model performance can drift as populations and conditions change.
Case Study Comparison: Traditional vs. ML Approaches
| Task | Traditional Method | ML Approach | Impact |
|---|---|---|---|
| Cooling tower identification | Manual satellite image review: 4 hours per area | TowerScout computer vision: 5 minutes per area | 98% time reduction |
| Disease surveillance | Case report aggregation: days to weeks delay | Real-time syndromic surveillance with ML | Immediate outbreak detection |
| Risk stratification | Simple scoring based on 3-5 factors | ML models integrating dozens of variables | AUROC 0.82 for bloodstream infection outcomes |
| News monitoring | Manual review of global health news | NewsScape NLP system | 80% faster with higher efficiency |
Research Priorities and Knowledge Gaps
Several areas need more work:
- Health equity applications: Only 105 of the ML publications analyzed focused on equity—a small percentage of the total. Methods for detecting and addressing algorithmic bias need development.
- Causal inference: Most ML models predict correlations but can’t prove causation. Public health needs to understand what drives outcomes, not just predict them.
- Small data settings: ML typically requires large datasets. Methods that work with limited data—common in resource-constrained settings or rare diseases—remain challenging.
- Interpretability: More research is needed on explainable AI methods that maintain predictive performance while showing how decisions are made.
- Implementation science: The technical ML literature is vast. Guidance on real-world deployment in public health contexts is scarcer.
Frequently Asked Questions
What’s the difference between machine learning and artificial intelligence in public health?
Artificial intelligence is the broader field of computer systems performing tasks that typically require human intelligence. Machine learning is a subset of AI focused specifically on algorithms that learn patterns from data. In public health, most practical AI applications currently use ML techniques—neural networks, random forests, support vector machines—rather than other AI approaches like expert systems or symbolic reasoning.
Can machine learning replace epidemiologists and public health workers?
No. ML amplifies what public health professionals can accomplish, but it doesn’t replace human judgment, contextual understanding, or ethical reasoning. Models require interpretation, validation requires domain expertise, and decisions affecting communities need human accountability. The most effective applications combine ML automation with expert oversight.
How accurate are ML models for disease prediction?
Accuracy varies by application and dataset. Ensemble models have achieved 92% accuracy for certain diseases like acute hepatitis B and malaria. Forecasting models for dengue and influenza reach up to 93% accuracy. Bloodstream infection outcome prediction achieved AUROC of 0.82. But these numbers come from controlled studies—real-world performance often drops when models face new populations or changing conditions. Continuous monitoring is essential.
What are the main ethical concerns with ML in public health?
Key concerns include algorithmic bias that worsens health disparities, privacy risks from large-scale data collection, lack of transparency in how decisions are made, potential for misuse or unintended consequences, and questions about accountability when algorithms err. Addressing these requires diverse training data, fairness audits, explainable models, strong governance, and community engagement in deployment decisions.
Do public health agencies need their own data scientists to use machine learning?
Not necessarily. Options include hiring data science staff, partnering with academic institutions, using commercial ML platforms designed for healthcare, or participating in shared services through state or federal programs. CDC’s AI Accelerator Program provides a model for developing and scaling AI solutions across multiple jurisdictions. The right approach depends on an agency’s size, budget, and strategic priorities.
How much does it cost to implement ML systems in public health?
Costs vary enormously based on scope. Cloud-based tools and open-source algorithms reduce infrastructure costs compared to building everything in-house. Staff time for data preparation, model development, and validation typically exceeds technology costs. CDC’s GenAI chatbot generated $3.7 million in labor savings with a 527% ROI, showing that strategic implementations can pay for themselves. Start with pilot projects to demonstrate value before large investments.
Can small health departments benefit from machine learning?
Yes, though resource constraints create challenges. Smaller departments can access ML capabilities through state or regional partnerships, vendor solutions, or federal programs. Focus on high-value applications where ML solves specific pain points—automated report screening, outbreak forecasting, resource optimization. Federated learning approaches allow collaboration without requiring local ML expertise at every site.
Conclusion
Machine learning is already transforming public health. CDC’s operational systems demonstrate measurable impact—98% time reductions, 527% return on investment, 80% efficiency improvements. These aren’t future possibilities. They’re happening now.
The applications span the full spectrum of public health work: surveillance that catches outbreaks in real time, diagnostic support that identifies at-risk patients earlier, resource allocation that targets limited capacity where it matters most, and equity analysis that reveals hidden disparities.
But ML is a tool, not a solution. It amplifies what skilled public health professionals can accomplish while introducing new challenges around bias, transparency, privacy, and equity. Success requires treating ML as part of a broader modernization strategy—one that includes data infrastructure, workforce development, ethical governance, and community engagement.
The research gaps are clear: health equity applications need expansion, causal inference methods need development, and implementation science needs more real-world guidance. Only a small percentage of publications focused on equity—a gap that must close.
For agencies considering ML adoption, start small. Identify a specific high-value problem. Build a multidisciplinary team. Validate rigorously. Monitor continuously. Learn from leaders like CDC who have demonstrated what works.
The next pandemic, the next outbreak, the next health crisis won’t wait for perfect systems. ML gives public health the speed, scale, and precision to protect populations in an increasingly complex threat landscape. The question isn’t whether to adopt these tools—it’s how to do so responsibly, equitably, and effectively.