Quick Summary: Machine learning is revolutionizing biomedical research by extracting patterns from complex biological data, accelerating drug discovery, and improving diagnostic accuracy. FDA-authorized AI medical devices now includes over 1,300 cleared devices, while NIH-funded projects demonstrate ML applications across imaging, genomics, and precision medicine. These technologies enable researchers to predict disease progression, optimize treatment selection, and uncover molecular insights that would be impossible through traditional analysis methods.
Biomedical data generation increases rapidly, with major datasets expanding substantially year over year. This explosive growth in health data has made traditional analysis methods increasingly inadequate for extracting meaningful insights.
Machine learning approaches have emerged as essential tools for making sense of this data explosion. From predicting drug responses to identifying cancer biomarkers, these algorithms are fundamentally changing how researchers approach biological questions.
The FDA now maintains a list of AI-enabled medical devices authorized for marketing in the United States, reflecting the rapid clinical translation of these technologies. Meanwhile, institutions like the National Institute of Biomedical Imaging and Bioengineering fund projects ranging from optoacoustic tomography to pediatric radiograph analysis.
But here’s the thing—not all machine learning applications in biomedicine look the same. The field spans everything from supervised classification of disease states to unsupervised discovery of cellular subtypes.
This guide breaks down how machine learning actually works in biomedical contexts, where it’s making the biggest impact, and what challenges researchers still face when implementing these approaches.
Understanding Machine Learning in Biomedical Contexts
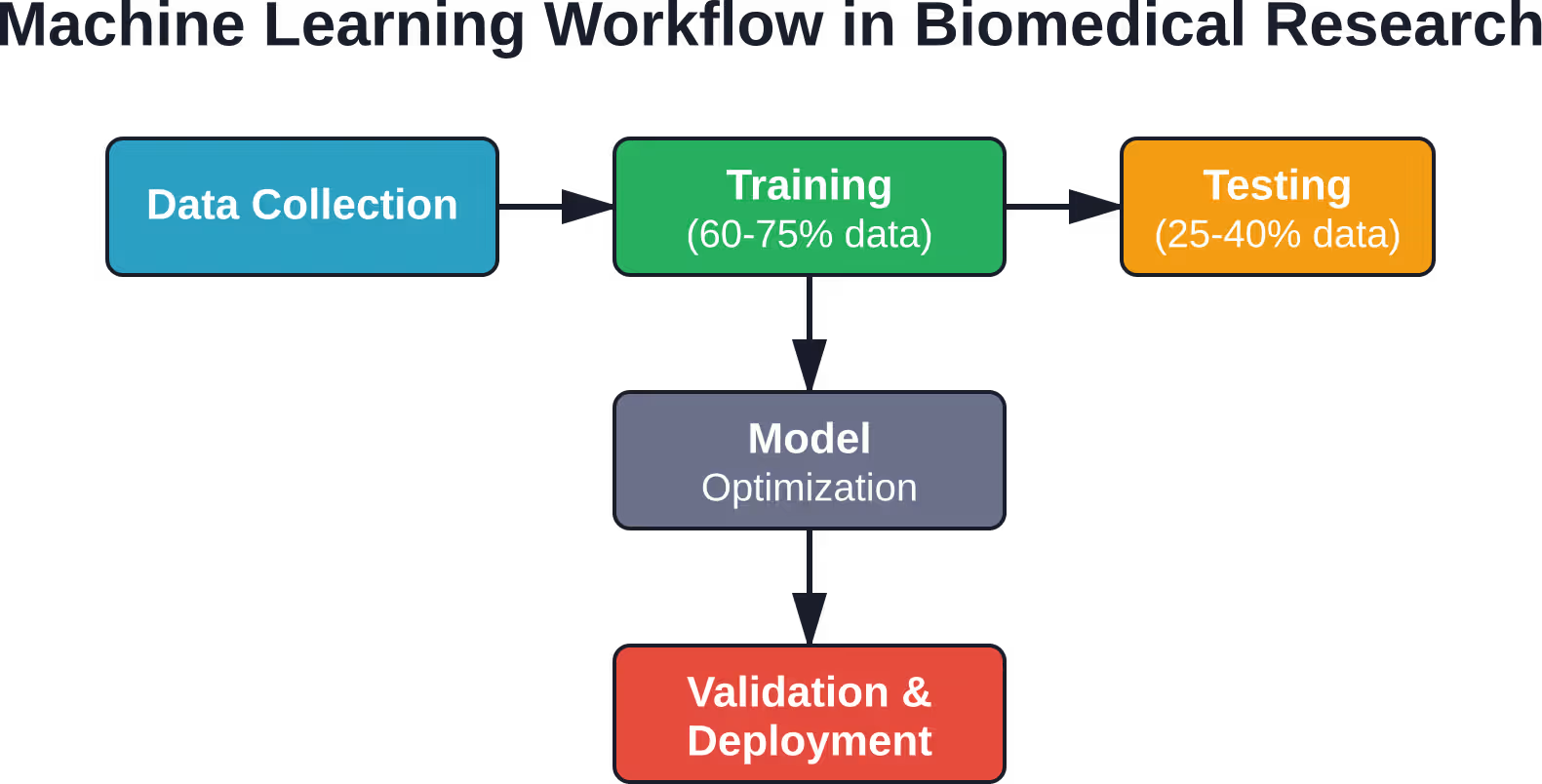
Machine learning algorithms attempt to extract patterns from data and associate those patterns with discrete classes or continuous outcomes. Unlike traditional statistical methods that require explicit programming of every rule, these systems learn from examples.
The basic workflow typically splits data into training and test subsets. The larger portion—often 60-75% of available data—trains the model, while the remaining subset evaluates predictive performance.
This approach matters in biomedicine because biological systems generate complex, high-dimensional data that defies simple analysis. Genomic sequencing produces millions of data points per sample. Medical imaging creates terabytes of pixel information. Electronic health records contain thousands of variables per patient.
Three Core Learning Paradigms
Supervised learning uses labeled training data where outcomes are known. A cancer classification model might train on biopsy images already categorized as malignant or benign. Once trained, it predicts classifications for new, unlabeled samples.
Unsupervised learning finds structure in unlabeled data without predetermined categories. Researchers might use clustering algorithms to identify patient subgroups based on gene expression patterns, discovering disease subtypes that weren’t previously recognized.
Reinforcement learning optimizes sequential decisions through trial-and-error interactions. In clinical contexts, this approach can identify optimal treatment sequences by learning from patient outcome trajectories.
Each paradigm suits different biomedical questions. The choice depends on available data, the research question, and whether ground truth labels exist.
Why Traditional Methods Aren’t Enough
Standard statistical approaches work well for hypothesis testing with controlled variables. But biomedical research increasingly confronts scenarios where traditional methods struggle.
Consider predicting cardiovascular disease risk. Hundreds of potential variables might matter—genetic markers, lifestyle factors, medication history, lab values, imaging features. Linear regression can’t capture the complex, non-linear interactions between these factors.
Machine learning algorithms excel at modeling these intricate relationships. Neural networks, for instance, automatically discover relevant feature combinations without researchers manually specifying every interaction term.
The algorithms also handle missing data and noise better than classical methods. Real-world medical data is messy—patients skip appointments, measurements contain errors, records are incomplete. Robust ML approaches account for this messiness.

Apply Machine Learning to Biomedical Research With AI Superior
Biomedical research generates complex and high-volume data that can benefit from structured machine learning analysis. AI Superior helps research teams turn raw biomedical data into actionable models, ensuring methods are robust, reproducible, and aligned with research goals.
They can assist with:
- Identifying research areas suitable for machine learning
- Reviewing and preparing datasets for model development
- Creating proof of concept models to test hypotheses
- Developing predictive, classification, or pattern recognition models for biomedical applications
- Evaluating model performance and optimizing reliability
- Integrating AI solutions into research workflows for improved decision-making
Machine learning applications in biomedical research include biomarker discovery, disease modeling, drug target prediction, patient stratification, and experimental data analysis.
Reach out to AI Superior to advance your biomedical research with machine learning.
Deep Learning Transforms Medical Imaging Analysis
Convolutional neural networks have achieved remarkable performance in analyzing medical images. These deep learning architectures automatically learn visual features without manual feature engineering.
The National Institute of Biomedical Imaging and Bioengineering funds projects demonstrating this capability. One research team developed CNN systems that automatically detect tumor areas within whole-slide images and calculate PD-L1 tumor proportion scores.
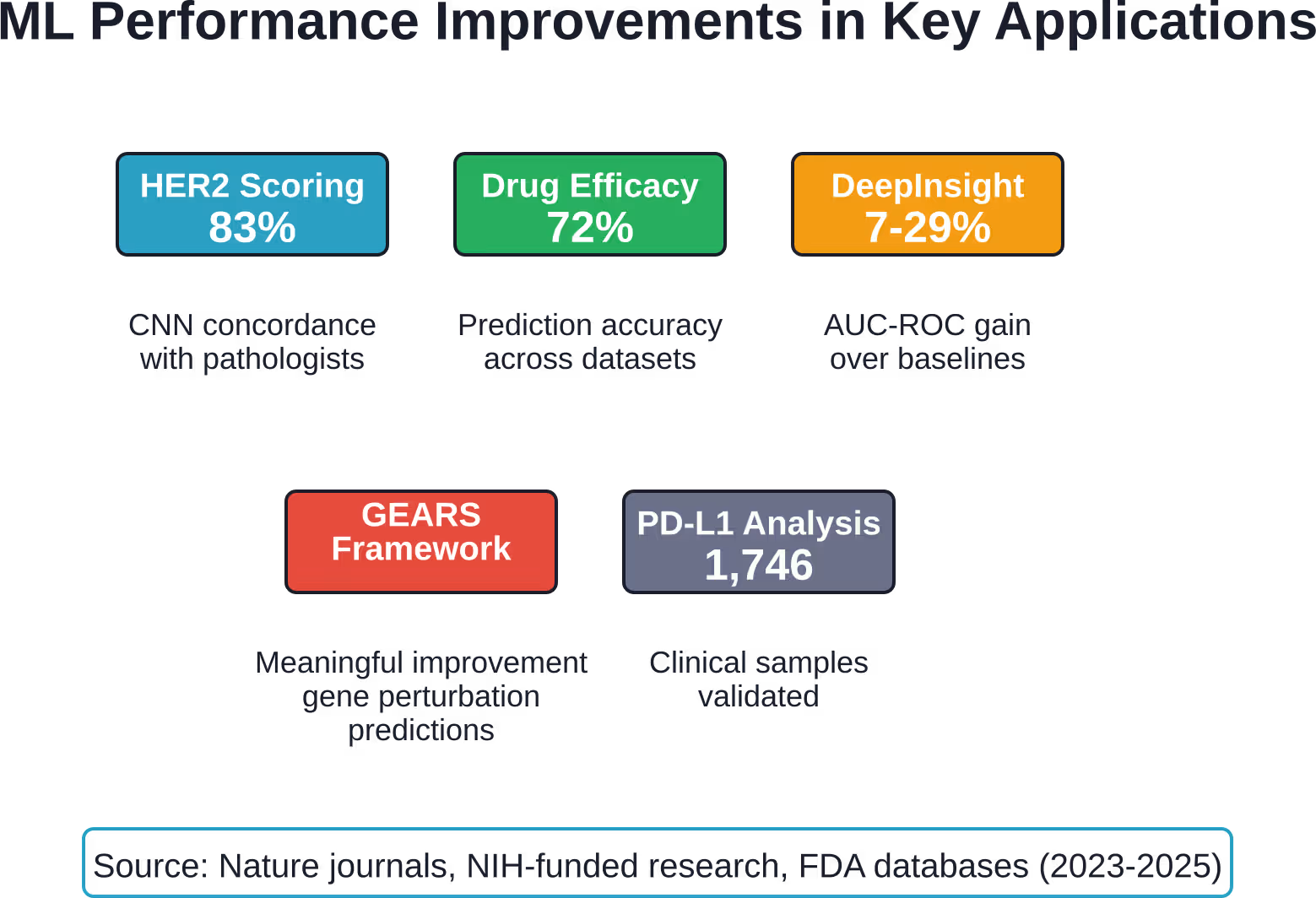
High concordance rates between CNN-based automated scoring and pathologist assessment have been reported across breast tumor samples. In cases where discordance occurred, independent pathologist review sometimes modified the initial assessment, suggesting the AI system provided valuable validation.
Breaking Down CNN Architecture
Convolutional neural networks process images through multiple layers of learned filters. Early layers detect simple features like edges and textures. Deeper layers combine these into complex patterns—cellular structures, tissue organization, abnormal growth patterns.
This hierarchical feature learning mirrors how visual processing works in biological systems. The approach proves particularly powerful for histopathology, radiology, and other image-intensive medical specialties.
One funded project focuses on optoacoustic tomography breast imaging using computational frameworks that enable virtual imaging trials. Another develops deep learning pipelines to assess peripherally inserted central catheters on pediatric radiographs.
The FDA’s evolving guidance on AI-enabled medical devices recognizes these advances while emphasizing the need for rigorous validation. Real-world performance monitoring matters because medical imaging systems encounter diverse patient populations and equipment variations.
From Research to Clinical Deployment
Translating imaging algorithms from research settings into clinical practice requires addressing several challenges. Model performance can degrade when applied to data from different institutions, imaging equipment, or patient demographics.
Transfer learning helps mitigate this issue. Models pre-trained on large image datasets can be fine-tuned with smaller institution-specific datasets, reducing computational costs while improving performance across varied clinical contexts.
Retrospective studies using data from clinical trials provide validation evidence. Analysis across CheckMate studies examined AI-based PD-L1 TPS classification for nivolumab and ipilimumab immunotherapy, demonstrating real-world applicability.
Precision Oncology Applications
Cancer treatment increasingly relies on molecular characterization of individual tumors. Machine learning accelerates the analysis of multi-dimensional omics data to identify therapeutic targets and predict treatment responses.
Machine learning models using multi-source cancer datasets have demonstrated promising accuracy for drug response prediction.
That accuracy matters because cancer treatments often fail due to tumor heterogeneity and resistance mechanisms. Predictive models help oncologists select treatments more likely to work for specific patients, avoiding ineffective therapies with significant side effects.
Spatial Pathology and Multiomic Integration
Tumors aren’t homogeneous masses. They contain diverse cell populations with distinct molecular profiles, spatial organization patterns, and microenvironmental interactions.
Modern ML approaches integrate spatial pathology data with genomics, transcriptomics, and proteomics. This multiomic analysis reveals how different tumor regions respond to treatment and which cellular neighborhoods drive disease progression.
One challenge involves the sheer complexity of these datasets. A single tumor sample might generate millions of gene expression measurements, thousands of protein quantifications, and detailed spatial maps of cellular organization.
Deep learning methods like DeepInsight transform tabular omics data into image-like representations that CNNs can process. This approach (DeepInsight-3D) showed 7–29% improvement in performance, as measured by model AUC-ROC, across baseline methods for tasks like cell type identification.
Predicting Treatment Resistance
Real talk: most cancer treatments eventually stop working. Tumors evolve, acquire resistance mutations, and develop escape mechanisms.
Machine learning models trained on longitudinal patient data can predict resistance before it becomes clinically apparent. These systems analyze patterns in serial biopsies, circulating tumor DNA, and imaging studies to identify early warning signs.
The GEARS framework demonstrated meaningful improvements in predicting transcriptional responses to multi-gene perturbations. While specific performance metrics vary across applications, this represents meaningful progress in understanding how tumors adapt to therapeutic pressure.
| Application Area | ML Approach | Key Advantage | Primary Challenge |
|---|---|---|---|
| Medical Imaging | Convolutional Neural Networks | Automated feature detection | Requires large annotated datasets |
| Drug Discovery | Graph Neural Networks | Molecular structure understanding | Validation in clinical trials |
| Genomics | Deep Learning (DeepInsight) | High-dimensional data handling | Biological interpretability |
| Disease Prediction | Ensemble Methods | Robust across data types | Integration with clinical workflow |
| Treatment Selection | Reinforcement Learning | Sequential decision optimization | Requires extensive outcome data |
Virtual Cell Models and Drug Development
AI-driven virtual cell models represent a paradigm shift in preclinical research. These systems integrate multimodal omics data with advanced algorithms to predict cellular responses to drugs and genetic perturbations.
The approach enables high-precision predictions of drug responses, gene perturbations, and disease progression without requiring extensive animal testing. Virtual cells can simulate how thousands of drug candidates might affect specific cell types or disease states.
Generative Models for Molecular Design
Deep generative models learn the rules governing molecular structure and biological activity. Once trained, they can generate novel molecular structures optimized for specific therapeutic properties.
This differs fundamentally from traditional drug discovery, which screens large libraries of existing compounds. Generative approaches create new molecules tailored to precise specifications—binding affinity, metabolic stability, minimal side effects.
Graph neural networks excel at this task because they naturally represent molecular structures as graphs, with atoms as nodes and chemical bonds as edges. The networks learn which structural motifs correlate with desired biological activities.
CRISPR Validation and Experimental Verification
Virtual cell predictions require experimental validation. CRISPR assays and organoid platforms provide that critical verification step.
Researchers can test whether predicted gene perturbation effects actually occur in laboratory models. This closed-loop workflow—computational prediction followed by experimental validation—accelerates research by focusing laboratory resources on the most promising hypotheses.
Organoids derived from patient cells offer particularly valuable validation platforms. They capture individual genetic backgrounds and disease characteristics, enabling personalized predictions about which treatments might work for specific patients.
The FDA recognizes this potential while noting that regulatory acceptance, data privacy protections, and model interpretability remain active challenges. Global policy trends emphasize standardization to enhance clinical translation.
Physics-Informed Machine Learning
A newer frontier combines machine learning with physics-based and biology-based modeling. Physics-informed machine learning embeds fundamental laws—often expressed as differential equations—into neural network architectures.
Why does this matter? Pure data-driven approaches sometimes violate known biological constraints. A model might predict negative cell counts or impossible metabolic rates because it learned statistical associations without understanding underlying mechanisms.
Physics-informed approaches enforce biological plausibility. The models learn from data while respecting conservation laws, mass balance equations, and biochemical kinetics.
Disease Progression Modeling
Predicting how diseases evolve over time requires modeling dynamic biological processes. Differential equations describe rates of change—tumor growth kinetics, viral replication dynamics, immune system responses.
Traditional mechanistic models require knowing exact parameter values, which often aren’t available. Physics-informed ML learns these parameters from patient data while maintaining the mechanistic structure that makes predictions biologically interpretable.
This hybrid approach proves especially valuable for personalized medicine. The models can be calibrated to individual patients using their historical data, then project forward to predict future disease states under different treatment scenarios.
Cardiovascular and Metabolic Applications
Cardiovascular disease involves complex hemodynamics governed by fluid mechanics equations. Machine learning models that incorporate these physical laws outperform purely data-driven approaches for predicting blood flow, vessel wall stress, and rupture risk.
Similarly, metabolic modeling benefits from physics-informed approaches. Glucose regulation, drug pharmacokinetics, and hormone dynamics all follow known biochemical principles that constrain the solution space for ML models.
The result is more robust predictions that generalize better to new patients and clinical scenarios. Models grounded in biological mechanisms don’t just memorize training data patterns—they capture transferable knowledge about how biological systems actually work.
Data Challenges and Preprocessing Requirements
Here’s what nobody tells you about machine learning in biomedical research: most of the work isn’t building fancy models. It’s wrangling messy, heterogeneous data into usable form.
Biomedical datasets contain missing values, measurement errors, batch effects, and inconsistent coding schemes. Electronic health records mix structured data with unstructured clinical notes. Genomic datasets from different sequencing platforms aren’t directly comparable.
Handling High-Dimensional Data
Omics studies routinely measure tens of thousands of variables on hundreds of samples. This creates the “curse of dimensionality”—when feature count exceeds sample size, models can memorize noise rather than learning signals.
Feature selection methods identify which variables actually contribute to predictions. Dimensionality reduction techniques like principal component analysis compress high-dimensional data into lower-dimensional representations while preserving important variation.
But wait. These preprocessing choices affect downstream results. Different normalization methods, batch correction approaches, or feature selection thresholds can lead to different biological conclusions.
Robust analysis pipelines use multiple preprocessing strategies and check whether key findings replicate across approaches. Sensitivity analysis reveals which results depend critically on specific methodological choices.
Addressing Data Heterogeneity
Biomedical data comes from diverse sources—academic medical centers, community hospitals, different countries, various patient populations. This heterogeneity challenges model generalization.
A model trained on data from one institution might perform poorly at another due to differences in patient demographics, clinical protocols, or equipment. Domain adaptation techniques help models transfer across contexts.
Multi-site studies that pool data from multiple institutions provide more representative training sets. Federated learning approaches enable collaborative model training without sharing sensitive patient data—algorithms travel to data rather than data traveling to algorithms.
Dealing with Missing and Imbalanced Data
Real clinical datasets have missing values. Patients miss follow-up appointments. Lab tests aren’t ordered. Records are incomplete.
Simple approaches like deleting incomplete records waste valuable data and can introduce bias if missingness correlates with patient outcomes. Imputation methods fill in missing values using information from similar patients or related variables.
Class imbalance poses another challenge. Rare diseases affect few patients, so datasets contain far more controls than cases. Models trained on imbalanced data often just predict the majority class for everything.
SMOTE-based data balancing approaches generate synthetic minority class examples to balance training sets. Cost-sensitive learning methods penalize misclassification of rare classes more heavily. Ensemble methods combine multiple models to improve minority class detection.
| Data Challenge | Impact on Models | Solution Approaches |
|---|---|---|
| Missing Values | Reduced sample size, potential bias | Imputation, multiple imputation, missingness as feature |
| High Dimensionality | Overfitting, poor generalization | Feature selection, dimensionality reduction, regularization |
| Class Imbalance | Poor minority class prediction | SMOTE, cost-sensitive learning, ensemble methods |
| Batch Effects | Technical variation masks biology | ComBat normalization, batch as covariate, deep learning correction |
| Data Heterogeneity | Poor cross-site generalization | Domain adaptation, federated learning, multi-site training |
Model Validation and Clinical Translation
Impressive performance on test sets doesn’t guarantee clinical utility. Models must demonstrate real-world effectiveness across diverse patient populations and healthcare settings.
The FDA emphasizes evaluating AI-enabled medical device performance in real-world contexts. Their guidance documents outline best practices for measuring and validating performance outside controlled research environments.
Validation Hierarchy
Internal validation uses held-out test data from the same cohort that provided training data. This establishes baseline performance but provides limited evidence of generalizability.
External validation tests models on completely independent datasets from different institutions or time periods. Strong external validation performance suggests the model captured generalizable biological patterns rather than institution-specific artifacts.
Prospective clinical validation deploys models in active clinical workflows and measures impact on patient outcomes. This represents the gold standard—does the AI system actually improve care?
Good machine learning practice for medical device development requires documentation of data sources, model architecture choices, training procedures, and validation results. Transparency enables reproducibility and facilitates regulatory review.
Interpretability and Clinical Acceptance
Clinicians reasonably hesitate to trust black-box predictions. Understanding why a model makes specific predictions builds confidence and enables identification of when models fail.
Attention mechanisms in neural networks highlight which input features drove particular predictions. For medical images, attention maps show which image regions influenced diagnostic classifications.
Feature importance analyses rank variables by their contribution to model predictions. Clinicians can assess whether models rely on medically sensible features or spurious correlations.
But here’s the challenge—complex models are complex for a reason. They capture intricate patterns that simple, interpretable models miss. The field continues grappling with the tradeoff between accuracy and interpretability.
Integration into Clinical Workflows
Technical performance matters less if systems don’t fit clinical workflows. Implementation requires addressing practical concerns—computational requirements, integration with existing electronic health records, user interface design, alert fatigue.
Successful deployments involve clinical experts throughout development. Clinicians help specify model requirements, select relevant features, interpret results, and identify failure modes.
Studies show clinical expert involvement occurs most frequently when specifications are made or implementations evaluated. However, clinicians are less prevalent in developmental stages for verifying clinical correctness or preprocessing data—suggesting opportunities to strengthen collaboration.
Ethical Considerations and Bias Mitigation
Machine learning systems can perpetuate or amplify biases present in training data. Healthcare data reflects historical inequities in access, treatment, and outcomes across demographic groups.
Models trained on biased data produce biased predictions. If training data under-represents certain populations, model performance degrades for those groups. If historical treatment decisions reflected prejudice, models may learn to replicate discriminatory practices.
Sources of Algorithmic Bias
Selection bias occurs when training cohorts don’t represent target populations. Academic medical center data over-represents patients with complex conditions who receive tertiary care.
Measurement bias arises from differences in how variables are measured across groups. Pulse oximetry, for instance, shows reduced accuracy in patients with darker skin tones—models using oxygen saturation readings may perform unequally.
Label bias happens when outcome definitions disadvantage specific groups. Using healthcare utilization as a proxy for health needs underestimates actual needs for populations facing access barriers.
Fairness-Aware Machine Learning
Addressing bias requires intentional intervention. Fairness-aware ML approaches include demographic parity (equal prediction rates across groups), equalized odds (equal error rates), and calibration (predictions mean the same thing across groups).
These fairness criteria sometimes conflict—optimizing for one may worsen another. Choosing appropriate fairness definitions requires considering specific clinical contexts and consulting affected communities.
Adversarial debiasing trains models to make accurate predictions while preventing them from inferring sensitive attributes like race or gender. Fairness constraints can be built directly into optimization objectives.
Post-processing methods adjust model outputs to satisfy fairness criteria. These approaches modify predictions to equalize error rates or calibration across groups while maintaining overall accuracy.
Data Privacy and Security
Biomedical data is sensitive. Machine learning systems must protect patient privacy while enabling research progress.
De-identification removes direct identifiers, but high-dimensional medical data remains vulnerable to re-identification. Combining genomic data with demographic information can uniquely identify individuals.
Differential privacy adds calibrated noise to data or model outputs, providing mathematical guarantees that individual records can’t be reverse-engineered from published results or deployed models.
Secure multi-party computation enables collaborative analysis across institutions without sharing raw data. Homomorphic encryption allows computations on encrypted data without decryption.
Regulatory frameworks like HIPAA in the United States and GDPR in Europe govern healthcare data usage. AI developers must navigate these requirements while pursuing research objectives.
Future Directions and Emerging Trends
The convergence of advancing technologies promises to accelerate biomedical discovery. Several trends are reshaping how machine learning approaches will evolve over the coming years.
Foundation Models for Biology
Large language models transformed natural language processing by training massive neural networks on enormous text corpora. Similar foundation models are emerging for biological sequences, molecular structures, and medical images.
These models learn general biological representations that transfer across tasks. A model pre-trained on millions of protein sequences can be fine-tuned for specific prediction tasks with minimal additional data—predicting protein function, stability, or interactions.
The approach democratizes access to powerful ML capabilities. Smaller research groups without resources to train massive models from scratch can adapt foundation models to their specific questions.
Multi-Modal Learning
Biological systems are inherently multi-modal—genomics, transcriptomics, proteomics, metabolomics, imaging, clinical variables all provide complementary information. Integrating these data types remains challenging.
New architectures specifically designed for multi-modal learning can process different data types simultaneously and learn how information from different modalities relates. Attention mechanisms weight the contribution of each modality for specific predictions.
Multi-modal models promise more complete biological understanding by capturing relationships that single-modality analyses miss. The genetic variant that matters might only be consequential in specific cellular contexts detectable through imaging.
Causal Discovery and Intervention
Most machine learning identifies correlations. But biological understanding requires knowing causation—what drives disease progression? Which interventions actually change outcomes?
Causal inference methods adapted for ML settings help distinguish correlation from causation in observational data. These approaches estimate what would happen under interventions even when randomized experiments aren’t feasible.
Reinforcement learning optimizes sequential treatment decisions by learning from patient outcome trajectories. These dynamic treatment regime algorithms can identify personalized strategies that adapt based on how patients respond.
Continuous Learning Systems
Current models are static—trained once, then deployed without further updating. But medical knowledge evolves. New diseases emerge. Treatment guidelines change. Patient populations shift.
Continuous learning systems update as new data becomes available, maintaining performance as clinical contexts change. The FDA’s evolving regulatory framework for AI-enabled medical devices with continuous learning capabilities reflects recognition of this paradigm shift.
The challenge involves maintaining safety and effectiveness while allowing adaptation. Systems must detect when substantial changes occur that warrant regulatory review versus routine updates within validated operating ranges.
Practical Implementation Considerations
Successful ML implementation requires more than algorithmic sophistication. Practical considerations around computational infrastructure, team composition, and project management determine whether research translates into impact.
Computational Infrastructure
Deep learning models require substantial computational resources. Training large neural networks demands high-performance GPUs and significant memory.
Cloud computing platforms provide scalable resources without upfront hardware investments. Academic researchers can access high-performance computing through institutional clusters or cloud credits from providers.
But infrastructure choices affect reproducibility. Documenting software versions, random seeds, and hyperparameters enables others to replicate analyses. Containerization approaches like Docker package entire computational environments.
Team Composition and Collaboration
Effective biomedical ML requires multidisciplinary expertise—domain knowledge in biology or medicine, statistical and computational skills, software engineering capabilities, clinical insight.
No single person masters all these areas. Successful projects bring together complementary expertise through genuine collaboration, not superficial consultation.
Clinicians should be involved from project inception through validation. Their input shapes appropriate problem formulation, identifies relevant features, interprets biological plausibility of results, and anticipates implementation challenges.
ML experts contribute methodological rigor, awareness of pitfalls, and technical implementation. Biologists provide mechanistic understanding and experimental validation capabilities.
Starting Points for Researchers
For biomedical researchers new to machine learning, several practical steps facilitate getting started. Python has emerged as the dominant language for ML, with extensive libraries (scikit-learn, TensorFlow, PyTorch) and educational resources.
Many universities offer workshops or courses covering ML fundamentals for life scientists. Online resources provide tutorials specifically addressing biomedical applications.
Starting with simpler methods before jumping to deep learning makes sense. Logistic regression, random forests, and support vector machines often provide strong baselines and build intuition about how ML works.
Publicly available datasets enable practice without requiring immediate access to novel data. Repositories contain genomic, imaging, and clinical datasets with established benchmarks.
Measuring Impact and Defining Success
Technical performance metrics—accuracy, AUC, F1 score—matter, but don’t fully capture clinical value. Success ultimately depends on whether ML systems improve patient outcomes, reduce costs, or enable discoveries that advance biological understanding.
Clinical Utility Beyond Accuracy
A diagnostic model might achieve 90% accuracy but still lack clinical utility if its predictions don’t change management decisions or if existing methods are nearly as accurate and less expensive.
Decision curve analysis evaluates clinical net benefit by comparing models to simple decision rules (treat all patients, treat no patients). This approach weights correct and incorrect predictions by their clinical consequences.
Cost-effectiveness analyses assess whether improved predictions justify additional expense. Rare disease screening, for instance, requires extremely high specificity to avoid overwhelming healthcare systems with false positives.
Research Acceleration Metrics
For discovery-focused applications, impact manifests through research acceleration. How much does ML reduce time to identify therapeutic targets? How many fewer experiments are needed to test hypotheses?
Virtual screening of millions of molecular candidates identifies promising drugs faster than physical testing. Predictive models prioritize the most informative experiments, reducing resource waste on low-yield approaches.
The closed-loop integration of computation and experimentation—predict, validate, refine—accelerates iterative research cycles that drive scientific progress.
Equity and Access Considerations
Impact assessments should consider who benefits from ML advances. Technologies that only work for well-represented populations or require expensive infrastructure exacerbate healthcare disparities.
Successful translation ensures benefits reach diverse communities, including under-resourced settings. This requires attention to computational requirements (can models run on available hardware?), data needs (do they generalize to varied populations?), and implementation barriers.
| Evaluation Dimension | Key Metrics | Clinical Relevance |
|---|---|---|
| Discrimination | AUC-ROC, sensitivity, specificity | Can the model distinguish outcomes? |
| Calibration | Calibration plots, Brier score | Do predicted probabilities match observed rates? |
| Clinical Utility | Decision curve analysis, net benefit | Does the model improve clinical decisions? |
| Fairness | Equalized odds, demographic parity | Does performance differ across groups? |
| Generalizability | External validation performance | Does the model work in different settings? |
Frequently Asked Questions
What’s the difference between machine learning and artificial intelligence in biomedical research?
Machine learning represents a subset of artificial intelligence focused on algorithms that learn patterns from data without explicit programming. AI is the broader concept of systems performing tasks that typically require human intelligence. In biomedical contexts, most current AI applications use machine learning techniques—neural networks, random forests, support vector machines—to analyze medical images, predict outcomes, or discover patterns in omics data. Deep learning, using multi-layered neural networks, forms another subset particularly effective for complex pattern recognition in imaging and sequence data.
How much data is needed to train biomedical machine learning models?
Data requirements vary enormously depending on task complexity, model architecture, and data dimensionality. Simple models like logistic regression might work with hundreds of samples, while deep learning approaches typically require thousands to millions of training examples for robust performance. Transfer learning reduces data needs by starting with models pre-trained on large datasets and fine-tuning with smaller task-specific datasets. High-dimensional omics data with thousands of measured variables generally needs hundreds to thousands of samples to avoid overfitting. The rule isn’t absolute—data quality, feature relevance, and problem difficulty all matter as much as raw sample count.
Can machine learning replace traditional biostatistics in medical research?
Machine learning complements rather than replaces traditional statistical methods. Classical statistics excels at hypothesis testing, estimating effect sizes with confidence intervals, and controlling for confounders—critical capabilities for understanding causation and making inferences from limited samples. ML shines at prediction tasks with complex, high-dimensional data where relationships are non-linear and interactions matter. Many successful biomedical studies combine approaches—using statistical methods for inference and causal understanding while employing ML for predictive modeling and pattern discovery. The choice depends on research questions and analytical goals.
How do researchers ensure machine learning models don’t perpetuate healthcare disparities?
Addressing bias requires intentional effort throughout model development. Training data should represent diverse populations proportionally to intended deployment contexts. Fairness-aware ML techniques explicitly optimize for equitable performance across demographic groups. Separate validation in underrepresented populations identifies differential performance that aggregate metrics might mask. Involving community stakeholders in defining appropriate fairness criteria ensures technical solutions align with ethical priorities. Post-deployment monitoring detects emerging disparities as patient populations or clinical practices evolve. Transparency about model limitations and performance variations across subgroups enables informed clinical decision-making.
What regulatory pathways do AI-enabled medical devices follow for FDA approval?
The FDA regulates AI-enabled medical devices based on risk classification and intended use. Lower-risk devices may qualify for 510(k) clearance by demonstrating substantial equivalence to predicate devices. Higher-risk devices require premarket approval with clinical evidence of safety and effectiveness. The FDA published guidance on good machine learning practice emphasizing transparency in development, robust validation, and risk management. For continuously learning systems that update post-deployment, the agency developed a regulatory framework balancing innovation with patient safety. Manufacturers submit predetermined change control plans describing anticipated updates and validation approaches. The FDA maintains a public list of authorized AI-enabled devices to foster transparency and innovation.
How long does it typically take to develop and validate a clinical machine learning model?
Development timelines span months to years depending on project scope, data availability, and validation requirements. Initial model development—problem formulation, data preprocessing, algorithm selection, training—might take several months for a focused research project. Rigorous validation extending to external datasets and prospective clinical evaluation adds substantial time, often one to two years or longer. Regulatory review processes add additional months. Academic research projects without immediate clinical deployment goals may proceed faster than commercial medical device development requiring FDA authorization. Data collection often represents the longest phase, particularly for prospective studies gathering patient outcomes over time. Successful translation from research prototype to deployed clinical system typically requires three to five years of sustained effort.
What programming skills are essential for biomedical researchers working with machine learning?
Python has emerged as the dominant language for biomedical ML due to extensive libraries (scikit-learn for classical ML, TensorFlow and PyTorch for deep learning, pandas for data manipulation, matplotlib for visualization) and active communities. R remains widely used for statistical genetics and bioinformatics with strong packages for genomic analysis. Beyond specific languages, foundational skills include data manipulation (reading files, handling missing values, merging datasets), statistical thinking (understanding bias-variance tradeoffs, cross-validation, hypothesis testing), and basic software engineering (version control with git, writing modular code, documentation). Many researchers successfully apply ML methods by learning programming alongside biomedical applications rather than mastering computer science fundamentals first. Collaborative teams combining programming expertise with domain knowledge often prove most effective.
Conclusion: The Path Forward
Machine learning has transitioned from experimental curiosity to an essential tool in biomedical research. The technologies enabling this transformation—increased computational power, massive datasets, algorithmic innovations—continue advancing rapidly.
Current applications already demonstrate meaningful impact. FDA-authorized AI medical devices assist clinicians with diagnostic imaging, risk prediction, and treatment planning. NIH-funded research projects push boundaries across drug discovery, precision medicine, and basic biological understanding.
But the field remains young. Substantial challenges around interpretability, fairness, validation, and clinical integration require sustained attention. Technical solutions alone won’t suffice—these problems demand multidisciplinary collaboration bringing together computational expertise, biological knowledge, clinical insight, and ethical reasoning.
The researchers who will drive progress understand both the tremendous potential and real limitations of machine learning approaches. They combine methodological sophistication with healthy skepticism, rigorously validating claims while pursuing ambitious applications.
Success requires meeting technical challenges—developing more robust algorithms, curating higher-quality datasets, improving interpretability. It equally demands addressing human and organizational factors—building collaborative teams, engaging stakeholders, navigating regulatory processes, ensuring equitable access to benefits.
The confluence of advancing technologies with evolving biological understanding creates unprecedented opportunities. Machine learning systems that integrate multimodal data, incorporate mechanistic knowledge, learn continuously from accumulating evidence, and provide interpretable insights will accelerate discovery and improve patient care.
For biomedical researchers, the imperative is clear: develop ML literacy sufficient to critically evaluate methods, identify appropriate applications, and collaborate effectively with computational experts. The alternative—ignoring these powerful approaches—means missing opportunities to answer important questions and advance human health.
The future of biomedical research is computational. Machine learning represents not just another tool in the methodological toolbox, but a fundamental shift in how biological questions are asked and answered. Researchers who embrace this transformation while maintaining scientific rigor will define the next era of biomedical discovery.
Ready to implement machine learning in your biomedical research? Start by identifying a specific, well-defined prediction or classification problem where substantial labeled data exists. Collaborate with computational experts early in project planning. Prioritize rigorous validation over impressive training performance. The path from prototype to clinical impact requires persistence, but the potential to transform patient care and scientific understanding makes the journey worthwhile.